-
Email info@ijcmcs.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
Digestive Surgery Department, Cho Ray Hospital, Vietnam.
*Corresponding author:Huan Nguyen Ngoc
Digestive Surgery Department, Cho Ray Hospital, Vietnam.
Email: waqarmazhar63@gmail.com
Received: Nov 05, 2024
Accepted: Dec 03, 2024
Published Online: Dec 10, 2024
Journal: International Journal of Clinical & Medical Case Studies
Copyright: © Ngoc HN (2024). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License
Citation: Ngoc HN. Familial adenomatous polyposis: A case report. Int J Clin Med Case Stud. 2024; 1(1): 1001.
Colon polyps, which are atypical growths on the colonic lining, exhibit significant variability in size, morphology, and risk for malignancy. Although numerous polyps are nonmalignant, several types possess the capacity to progress into colorectal cancer over time. When numerous colon polyps are identified, particularly in high-risk individuals or those with Familial Adenomatous Polyposis (FAP), a predominant genetic syndrome marked by aberrant cell proliferation, its most prevalent manifestation is the formation of extensive colorectal adenomas, ranging from hundreds to thousands. Surgical intervention may be required to excise these tumors and reduce the risk of cancer progression. We present a clinical case of a 31-year-old male admitted to the Digestive Surgery Department at Cho Ray Hospital with gastrointestinal complaints: constipation, persistent abdominal discomfort, and intermittent rectal hemorrhage. The colonoscopy findings revealed many polyps in the colon. Histological analysis verified the presence of a tubular adenoma with low-grade dysplasia. The patient underwent laparoscopic total proctocolectomy for the treatment of colon polyps, accompanied with ileoanal anastomosis and ileostomy. The patient was discharged home seven days after surgery, without complications. Surgical surgery for numerous colon polyps or familial adenomatous polyposis can diminish the risk of colorectal cancer. The objective is to efficiently excise polyps and avert their progression to malignancy, utilizing minimally invasive methods such as endoscopic polypectomy, endoscopic colectomy, or total colectomy.
Familial Adenomatous Polyposis (FAP) is a hereditary condition marked by the presence of multiple adenomatous polyps in the gastrointestinal mucosa, resulting in an almost 100% lifetime risk of Colorectal Cancer (CRC) and an incidence rate of between 1 in 7,000 to 1 in 30,000 live births [1,2]. Both male and female possess an equal likelihood of contracting the condition, independent of the parents’ gender, with an average onset occurring after 15 years [3]. Prior to this age, the condition is documented as asymptomatic and devoid of any signs [4].
FAP often arises from a germline pathogenic mutation in the Adenomatous Polyposis Coli (APC) tumor suppressor gene located on chromosome 5 [5]. This mutation mostly results in the formation of over 100 colorectal adenomatous polyps [6]. Most patients usually do not have symptoms, but they may present with diarrhea, rectal bleeding, abdominal pain, nausea, and obstruction, typically occurring in the age group of 20 to 30 years [7].
The risk of developing colorectal cancer is approximately 87% when the patient reaches 45 years of age. Patients who are not treated will have a risk of dying from colon cancer before the age of 40. The disease is often detected in the symptomatic stage due to blood in the stool. The best treatment method is a total colectomy with ileorectal anastomosis. In the case of malignant changes in the rectum, a total colectomy and a complete rectal resection with an ileostomy are necessary.
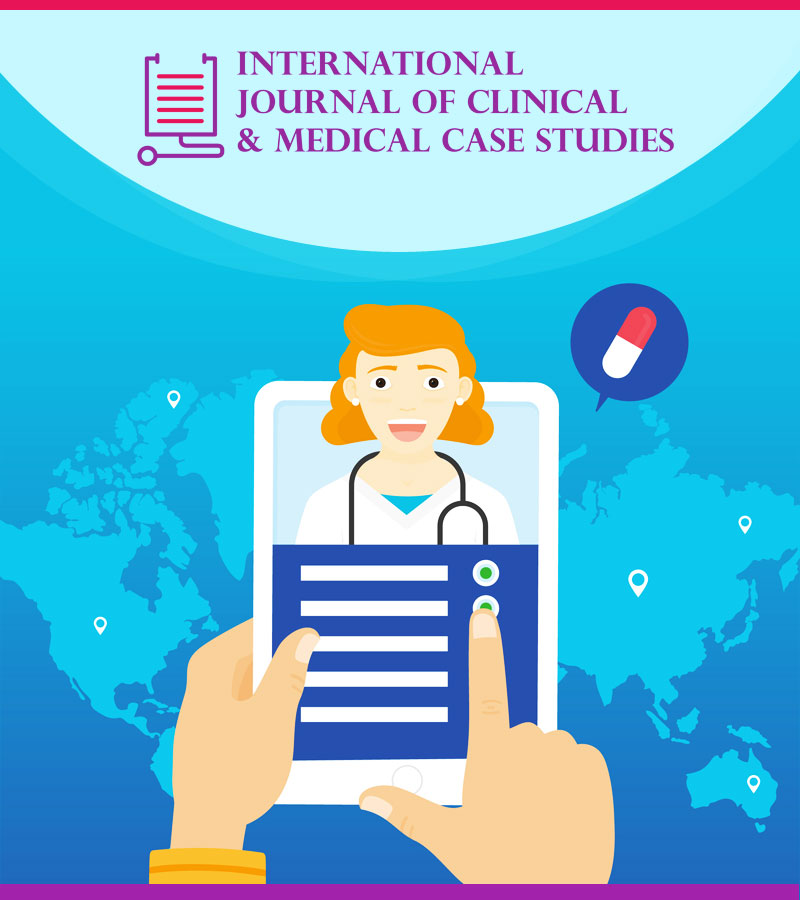
The patient is a 31-year-old male, admitted to the gastrointestinal surgery department with digestive issues: constipation, persistent abdominal pain, and occasional rectal bleeding. Upon examination, the patient showed no special signs. Blood tests show that the patient has mild anemia: RBC: 3.3 T/L; HGB: 105 g/L; HCT: 30%; WBC: 7.3 g/L; CEA 4 ng/ml. The colonoscopy results show multiple polyps in the colon (Figure 1).
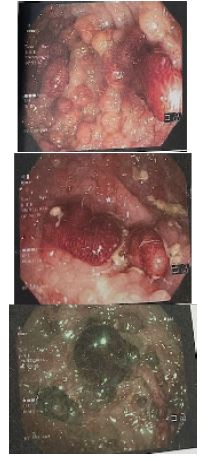
Histological examination confirmed tubular adenoma with low-grade dysplasia. Abdominal and pelvic CT normal. After discussing the treatment method with the patient and their family, the patient underwent laparoscopic total colectomy with multiple polyps, ileoanal anastomosis, and the ileal stoma was brought to the skin to protect the anastomosis. After the surgery, the colon was opened and examined, revealing numerous polyps covering the entire colonic mucosa (Figure 2).

The surgery duration was 262 minutes, with a blood loss of 125 ml, and the time to pass gas was 3 days. The patient was given sugar water on the first day after surgery and solid food on the second day after surgery. After 7 days in the hospital, with no complications, the patient was discharged home. The patient was re-examined after 1 month with stable clinical symptoms. Three months after the first surgery, the patient was hospitalized to close the ileostomy. The patient was discharged from the hospital 5 days after the surgery. Regular follow-up every 3 months and no abnormal signs within 1 year.
Familial Adenomatous Polyposis (FAP) is an autosomal dominant condition with great penetrance, impacting both genders equally. Approximately 20-30% of cases may result from de novo mutations, while the majority of affected individuals has a familial history of FAP syndrome [8]. The patient’s father had a comparable illness; however, there have been no indications of the sickness in the other siblings to date. CT scans and colonoscopy are essential for diagnosing and assessing rectal bleeding, particularly in young patients with high-risk factors such anemia and a substantial family history [9]. The diagnosis in our instance was performed with abdominal CT and colonoscopy to evaluate rectal bleeding, anemia, and a familial history of relatives with numerous colorectal polyps. The formation of many adenomatous polyps in the colon and rectum, commencing at birth and nearly invariably advancing to colorectal cancer by age 40, is a defining feature of FAP [6]. The diagnosis in our instance was definitively established following the study of the resected colon, which revealed over 1000 polyps without any malignant alterations in the adenomas. Molecular characterization of APC is essential to validate the diagnosis of FAP [6]. Accurate diagnosis of FAP necessitates extensive sampling of polyps for pathological examination and germline mutation testing, in conjunction with thorough evaluations of clinical manifestations, endoscopic images, and genetic tests, rather than solely depending on the presence or absence of adenomatous polyps [10]. Annual screening for classic Familial Adenomatous Polyposis (FAP) via flexible sigmoidoscopy or colonoscopy often commences at ages 10 to 12. Consequently, among individuals with Familial Adenomatous Polyposis (FAP), screening colonoscopy coupled with prompt intervention for detected lesions has resulted in a 55% decrease in the colorectal cancer incidence, marking the initial indicator of enhanced survival rates for patients [11]. The patient’s family members are uninformed of the ailment and the possible cause of the father’s death.
Surgery is fundamental in the management after FAP is diagnosed, and standard surgical options include total colectomy (with a Brooke ileostomy or ileal pouch-anal anastomosis) and subtotal colectomy with ileo-rectal anastomosis [12]. Indications for colectomy include symptomatic polyps, advanced adenomas including CRC, severe or progressive polyps, polyposis burden that cannot be effectively managed by endoscopy, or when surveillance is not possible [13]. Especially in young patients with a long-life expectancy and no progressive dysplasia and/or cancer, prophylactic surgery with Ileorectal Anastomosis (IRA) allows for rectal preservation and should be considered to enhance quality of life without affecting prognosis [14]. For prophylactic purposes, endoscopic total proctocolectomy -IRA is safe and feasible in young patients with low complication risk and good outcomes [15]. Our patient underwent total rectal resection via laparoscopy with ileal pouch-anal anastomosis due to polyps even in the rectum, along with loop ileostomy.
The risk of upper gastrointestinal cancer and desmoid tumors in patients with FAP remains present even after colectomy, leading to postoperative morbidity or reduced lifespan [16]. To assess the anastomosis site, pouch, and remaining rectum, it is recommended to perform endoscopic/colonoscopy procedures regularly after surgery every 6-12 months [17]. In the case of residual rectum, annual monitoring is very important [18]. Our patients are monitored and supervised regularly. Additionally, individuals with first-degree relatives known to have FAP, patients with more than 10 to 20 intestinal polyps, and/or patients with colonic adenomas associated with extraintestinal manifestations related to FAP are at high risk for FAP and should discuss testing [13]. None of the family members in our case have undergone any genetic testing so far and are also reluctant to undergo any genetic testing considering the family’s financial situation.
Managing patients with FAP is essential to ensure screening and appropriateness for these complex cases. Early colonoscopic screening is essential to determine the appropriate timing for surgical resection. Although medical treatments can provide good support, the main method in treating FAP is colectomy with or without proctectomy. Extraintestinal manifestations also require thorough screening recommendations with close clinical follow-up for patients with FAP. With monitoring and surgical removal, patients with FAP can significantly reduce the risk of colorectal cancer and other related malignancies. Laparoscopic surgery for the treatment of multiple colon polyps appears feasible and safe, with a low complication rate. When the techniques and instruments for endoscopic colon surgery are perfected, this procedure could become an attractive option for managing patients with multiple colon polyps.
Conflict of interest: No.
Funding: No.