-
Email info@ijcmcs.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Department of Burn and Plastic Surgery, Suzhou Hospital Affiliated to Nanjing Medical University, China.
2Department of Ultrasonography, Suzhou Hospital Affiliated to Nanjing Medical University, China.
*Corresponding author: Jian-Dong Su
Department of Burn and Plastic Surgery, Suzhou
Hospital Affiliated to Nanjing Medical University, Suzhou 215000, Jiangsu, China.
Email: jiandongsu@njmu.edu.cn
Received: Jan 24, 2025
Accepted: Feb 10, 2025
Published Online: Feb 17, 2025
Journal: International Journal of Clinical & Medical Case Studies
Copyright: © Jian-Dong S (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License
Citation: Xiao-Jun L, Xue-Ting Y, Min S, Jun Z, Jian-Dong S. Measurement to the paraumbilical perforator of deep inferior epigastric artery and estimation of its anatomical boundary by color ultrasound. Int J Clin Med Case Stud. 2025; 2(1): 1010.
Objective: To investigate the distinguishment of paraumbilical perforator of Deep Inferior Epigastric Artery (DIEA) between the diabetics and normal patients and estimate its anatomical district by color doppler ultrasound.
Methods: Fifteen people with wounds were divided into an observation group and a control group, according to their diabetic history (more than 5 years if they suffered). Both groups were carried out CDUS inspection before operations. We detected the perforator vessels to compare their calibration, Peak Systolic Velocity (PSV) and their length. We selected the potent perforator to estimate its anatomical boundary.
Results: The mean calibration of inferior epigastric artery with CDUS in diabetic group was less than the control group (P<0.05). While the difference of in-radium, PSV and comparative length of potent perforator between the observation group and control group was not significant. The mean Lenth of the perforator was about 5.5 cm.
Conclusion: Though the in-radium, PSV and comparative length of perforator hasn’t been detected decrease obviously, we found the calibration of DIEA in diabetics was reduced, which would affect the blood support and induce the flap’s necrosis.
Keywords: Perforator flap; Ultrasonic detection; Wound repair; Choke vessels.
The concept of perforator flap was first introduced in 1989. These are island flaps of subcutaneous tissue supplied by perforating arteries and veins, falling under the category of axial flaps [1]. Compared to traditional axial flaps, perforator flaps are more world widely used in reconstructive surgery. However, precise judgment by plastic surgeons is still required for selecting the appropriate perforator vessels and determine the size and length of the flap to avoid distal ischemic necrosis. Preoperative assessment of perforator vessels, including their localization, and estimation of both their length and blood supply area, remains crucial for the design and successful harvesting of the flap. Taylor and Saint-Crystal introduced the concepts of angiosomes, perforasomes, and choke zones at the edge of perforator flaps [2,3]. These concepts are primarily based on anatomical studies using static X-ray imaging with lead-containing dye perfusion in fresh cadavers. However, there is no literature providing ultrasound measurement data or elucidating the differences between diabetic patients and the normal population [4,5]. In this study, Color Doppler Ultrasound (CDUS) has been employed to measure the perforator vessels in the paraumbilical region of the abdominal wall in patients requiring wound repair. Relevant parameters such as the length, internal diameter, and flow velocity of the perforator vessels were collected. Patients were divided into diabetic and non-diabetic groups for comparison on the basis of their diabetic status, allowing for the observation of differences in perforator indicators and the evaluation of the anatomical supply area of the perforator flap.
Study subjects From July 2021 to October 2023, 15 patients were hospitalized at Suzhou Hospital Affiliated to Nanjing Medical University. The patients, aged between 20 and 64 years with an average age of 44.26 years, included 7 cases of upper limb defects repaired with pedicled inferior epigastric artery perforator flaps and 8 cases of patients with diabetes complicated by chronic wounds. General information about the patients is presented in Table 1. Among the patients, there were 14 males and 1 female. These patients included 3 cases of electrical injuries, 2 cases of thermal crush injuries, 1 case of deep burns and lacerations, 1 case of explosion injury, and 8 cases of diabetes complicated by chronic wounds. Inclusion criteria: (i) Age between 18 and 70 years; (ii) Patients with skin and soft tissue defects due to various causes who require repair using skin grafts or flaps. Exclusion criteria: (i) Patients with known dysfunction of the heart, lungs, kidneys, etc.; (ii) Patients with a history of bilateral abdominal wall surgery; (iii) Patients with hereditary vascular diseases; (iv) Patients unable to cooperate with ultrasound examinations. Due to the non-invasive nature, no side effects, and low cost of ultrasound examination of the abdominal wall, all patients agreed to undergo preoperative ultrasound examinations of the abdominal wall and signed informed consent forms. This study has been approved by the Branch for Clinical Technology Application, Ethics Committee of Suzhou Hospital Affiliated to Nanjing Medical University, with the ethics approval number: KL901188.
| No. | Gender | Age (years) | Diagnosis | |
|---|---|---|---|---|
| Diabetic group | 1 | Male | 63 | Diabetic foot |
| 2 | Male | 47 | Diabetic foot | |
| 3 | Male | 62 | Chronic skinulcer | |
| 4 | Male | 53 | Diabetic foot | |
| 5 | Male | 64 | Diabetic foot | |
| 6 | Male | 57 | Burns on both feet;diabetes | |
| 7 | Male | 44 | Diabetic foot | |
| 8 | Male | 32 | Inhalation injury; diabetes | |
| Control group | 1 | Male | 32 | Electrical injuryto the left hand |
| 2 | Male | 44 | Electrical injuryto both hands | |
| 3 | Male | 43 | Lecerations on the righthand | |
| 4 | Male | 20 | Explosion injuryto the lefthand | |
| 5 | Male | 36 | Hydrofluoric acisburn on the left hand | |
| 6 | Male | 30 | Electrical injuryto the left hand and chest | |
| 7 | Female | 37 | Thermal crush injury to the right middle finger |
Instruments and methods
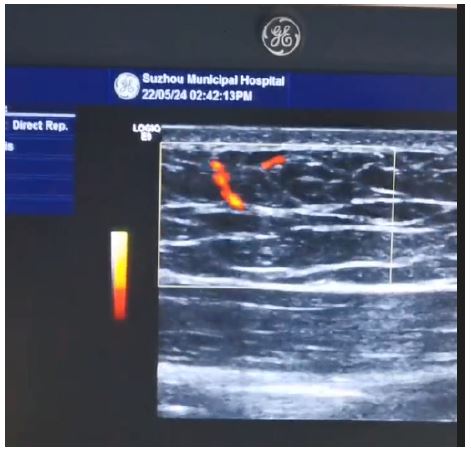
Instruments: A GE Logiq9 ultrasound diagnostic instrument was used. Vascular examination conditions included a linear array probe with a frequency of 8–12 MHz. The parameters were adjusted to the most sensitive settings without generating noise and then fixed (Figure 1).
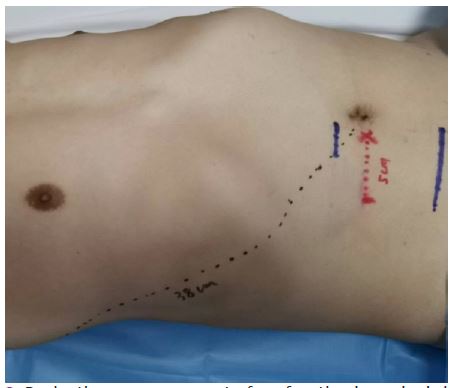
Patients were placed in a supine position with one side of the abdominal wall selected. The examination area was defined with the upper boundary 2 cm above the umbilicus, the lower boundary 6 cm below the umbilicus, the medial boundary along the midline of the abdomen, and the lateral boundary along the anterior axillary line. With coupling gel applied, the probe was used to gently press the skin to locate the inferior epigastric artery (with its internal diameter measured 6 cm below the umbilicus) and then trace the course of the vessel upward to find perforators. According to the commonly used oblique outward and upward design direction for paraumbilical flaps, the larger perforators in the outward or outward-upward direction were selected, and their diameter and Peak Systolic Velocity (PSV) were measured. The course of the perforating vessels was observed. When the perforator penetrated from the deep fascia, it was marked perpendicularly on the skin as point a, and when the perforator approached the entry point into the skin, it was marked as point b. The length of the line segment ab was the projection length of the perforator on the body surface (measurements are shown in Figure 2 and Figure 3). All these procedures were performed by the same ultrasound physician to ensure consistency in measurements and quality control. According to the measurement values, the dominant perforator with a larger internal diameter, higher flow velocity, and greater length was selected as the pedicle vessel for designing the interregional flap. In this group, a total of 15 cases were measured, and the results are recorded in Table 2.
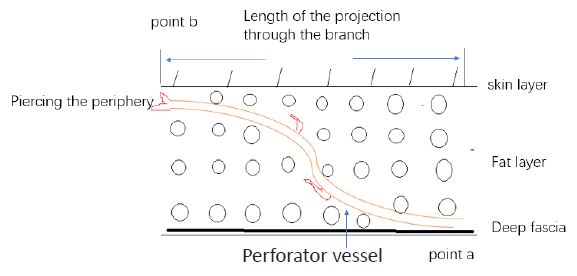
Point a was marked when the perforating branch penetrated the deep fascia, point b was marked as the position where the ultrasonic image basically disappeared when the perforating branch approached the skin layer while walking subcutaneously, and the length of line ab was the measured length of the perforating branch.
Statistical methods: SPSS 25.0 statistical software was used to analyze and process the perforator diameter, flow velocity, and perforator length, represented as mean ± standard deviation (x±s). Intergroup comparisons were performed through the independent samples t-test, with P< 0.05 considered statistically significant.
| Diabetic group | No. | Internal diameter of the inferior epigastric artery | Flowvelocity | Perforatorinternal diameter | Perforator flow velocity | PerforatorLength | From the umbilicus to the anterior axillary line | Relative perforatorlength |
|---|---|---|---|---|---|---|---|---|
| 1 | 2.3 | 23 | 1.5 | 20 | 4.20 | 8.50 | 0.49 | |
| 2 | 2.1 | 33.4 | 1.5 | 23.7 | 4.50 | 11.00 | 0.41 | |
| 3 | 3.2 | 40 | 2.1 | 34 | 4.50 | 9.00 | 0.5 | |
| 4 | 2.8 | 40 | 2.4 | 35 | 4.00 | 13.00 | 0.31 | |
| 5 | 1.3 | 33.6 | 0.6 | 18 | 6.50 | 14.00 | 0.46 | |
| 6 | 1.9 | 26.9 | 1.2 | 18.6 | 7.20 | 16.00 | 0.45 | |
| 7 | 3.4 | 40 | 2.2 | 36 | 5.00 | 14.00 | 0.36 | |
| 8 | 2.2 | 29 | 1.8 | 33 | 4.50 | 11.50 | 0.39 | |
| Control group | No. | Internal diameter of the inferior epigastric artery | Flowvelocity | Perforatorinternal diameter | Perforator flow velocity | PerforatorLength | From the umbilicus to the anterior axillary line | Relative perforatorlength |
| 1 | 2.5 | 40 | 2.1 | 36 | 7.0 | 16 | 0.43 | |
| 2 | 2.1 | 39 | 1.7 | 35 | 5.0 | 10 | 0.5 | |
| 3 | 2.2 | 74.2 | 1.2 | 28.4 | 10.0 | 11 | 0.91 | |
| 4 | 2.3 | 33 | 1.5 | 29 | 6.0 | 12 | 0.5 | |
| 5 | 1.9 | 32.7 | 1.2 | 29.4 | 7.0 | 13 | 0.54 | |
| 6 | 2.4 | 30 | 1.2 | 22 | 4.0 | 12 | 0.33 | |
| 7 | 1.7 | 32.5 | 0.9 | 21 | 4.0 | 11 | 0.36 | |
| P-value | 0.049 | 0.31 | 0.32 | 0.05 | 0.18 | 0.26 | 0.19 |
| Single-sample t-test confidence intervals | |||||
|---|---|---|---|---|---|
| Count | Sample | average value | standarddeviation | Standarderror | 95% CI |
| Value | 15 | 5.56 | 1.7 | 0.439 | 4.619 ~ 6.501 |
In the 15 patients studied, Color Doppler Ultrasound (CDUS) revealed that the internal diameter of the inferior epigastric artery in the diabetic group was smaller compared to the control group, and this difference was statistically significant (P<0.05), as shown in Table 2. In patients with diabetes, the internal diameter, flow velocity, and relative length of the dominant paraumbilical perforator did not show significant reduction compared to the control group (P>0.05). The average perforator length among the 15 patients was calculated to be 5.56 cm, with a 95% confidence interval of 4.6 to 6.5 cm, as shown in Table 3.
Flap transplantation is a primary method for repairing deep wounds and reconstructing body surface organs. Classified by blood supply, flaps can be random or axial, with axial flaps further divided into large-diameter known artery flaps and smaller-diameter perforator flaps (typically less than 0.8 mm in diameter). As this technique has developed, perforator flaps have become widely used due to several advantages, including the rich blood supply from perforating vessels, preservation of the main vascular trunks in the supply area, and reduced muscle damage [6].
In 1983, Taylor reported that the Paraumbilical Perforator flap (PUP) could be harvested with dimensions up to 42 cm by 16 cm, making it suitable for addressing large soft tissue defects in the upper limb [7]. Subsequently, the anatomy and clinical application of paraumbilical perforator flaps have become increasingly widespread. Blondeel et al. measured the paraumbilical perforators of the inferior epigastric artery, finding that perforator points with a diameter greater than 0.5 mm are primarily located within a quadrilateral area extending from 2 cm above to 6 cm below the umbilicus, and 6 cm to either side of the umbilicus [8]. Paraumbilical perforators can be classified as indirect or direct. Indirect perforators (diameter ≤0.5 mm) branch immediately after passing through the anterior sheath of the rectus abdominis and travel within the deep abdominal fat. Direct perforators (diameter ≥0.5 mm) run toward the skin, parallel to the skin surface above Scarpa’s fascia, and branch into the subdermal vascular network [9]. It is generally believed that as long as the subcutaneous vascular plexus is not damaged, the extensive vascular network it forms can ensure adequate blood supply to flaps. Shimin Zhang et al. believe that choke vessels are the connections formed between the branches of adjacent perforator vessels. There are 3 types of anastomoses: (1) true anastomoses without a reduction in diameter; (2) obstructive anastomoses with gradually decreasing diameters; (3) potential anastomoses that remain unopened under normal conditions [82]. However, the area of a perforator flap supplied by a single source artery is relatively small. In a given angiosome, perforator vessels branch out in a tree-like pattern as they travel toward the skin. The microvascular network in the subcutaneous plexus between adjacent perforasomes often has small diameters and may not open promptly, affecting blood supply. Therefore, in large perforator flaps spanning multiple regions, the potential supply area (choke zone) is prone to necrosis after flap harvesting [10,11].
The design axis of the paraumbilical perforator flap often extends from the paraumbilical perforator point to the ipsilateral inferior angle of the scapula [12]. In this context, we selected perforators oriented laterally or in the superolateral direction as the primary focus for measurement. According to the concepts of angiosomes and perforasomes proposed by Taylor and Crystal, an angiosome resembles a tree-like structure in three-dimensional form. However, the spatial structure of blood vessels after they perforate the deep fascia is represented by perforasomes. Between two adjacent perforasomes, the vessels theoretically have smaller diameters and lower density, which can be referred to as the choke zone of the angiosome [13,14]. This corresponds to the anatomical supply area. In ultrasound imaging, this can be approximated as the region where the perforator, while supplying blood to the skin, becomes gradually undetectable in the subcutaneous or near-dermal layer. This concept serves as the primary basis for measuring the length of abdominal wall perforators. The average perforator length measured was 5.56 cm, with a 95% confidence interval of 4.6 to 6.5 cm. The estimated anatomical supply area of the DIEAP flap extends approximately 5.5 cm or slightly further laterally from the perforator point (as indicated by the red line in Figure 2).
Compared to ultrasound, CTA has higher spatial resolution and can detect perforator vessels with a diameter of approximately 0.3 mm. Micro-CT scanning can extract the central axes of continuous perforator trunks and their branch network vessels, allowing for the cumulative addition of their lengths to determine the total vessel length. This method also indirectly reflects the continuity and density of the microvascular network in the flap, forming a measure of vascular connectivity density. After 3D reconstruction, detailed anatomical information about the perforator vessels can be clearly displayed, including their presence, quantity, exit location through the fascia, diameter, and subcutaneous course. However, ultrasound measurement is more intuitive and economical, and it also has a high sensitivity for measuring the internal diameter and flow velocity of blood vessels [15]. At the same time, in vivo ultrasound measurements are likely to differ from cadaveric angiographic studies due to factors such as blood flow. Ultrasound measurements should be considered closer to the actual physiological situation, as they are performed while the patient’s circulation and blood vessels are in a normal physiological state.
In diabetic patients, peripheral vessels often undergo hyaline degeneration and sclerosis, which may reduce the blood supply range of perforator vessels. According to the measured data, the internal diameter of the inferior epigastric artery is significantly smaller compared to the normal control group (P<0.05). This suggests a higher likelihood of atherosclerosis in diabetic patients, leading to narrowed lumens, and that the inferior epigastric artery may also be affected. In this study, no significant differences were found in the measured parameters (internal diameter, flow velocity, perforator length) of the dominant paraumbilical perforators of the DIEA in diabetic patients. We consider that this may be due to the small sample size, large individual differences, and variations in abdominal wall width and thickness, which can affect the measurements. Additionally, differences in ultrasound measurement techniques and diagnostic quality may contribute to the lack of significant findings. Future studies should aim to increase the sample size and standardize measurement methods to continue accumulating data.
The pedicled transfer of an inferior epigastric artery perforator flap is a common method for repairing deep distal upper limb wounds. When the flap harvest area is large, crossing the choke zone of perforator vessels can lead to distal flap necrosis. Using ultrasound to detect the internal diameter, flow velocity, and length perforators can provide a preliminary estimate of the blood supply range. Ultrasound measurement is an accurate, simple, and cost-effective screening method, and it is worth implementing routinely before perforator flap surgery.