-
Email info@ijcmcs.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Department of Hematology, Faculty of Graduate College, Kassala University, Kassala, Sudan.
2Department of Hematology, Faculty of Medical Laboratory Sciences, Port Sudan Ahlia University, Port Sudan, Sudan.
*Corresponding author: Bashir Abdrhman Bashir
Department of Hematology, Faculty of Medical Laboratory Sciences, Port Sudan Ahlia University, Port Sudan, Sudan.
Email: bashirbashir17@hotmail.com
Received: Jan 17, 2025
Accepted: Feb 12, 2025
Published Online: Feb 19, 2025
Journal: International Journal of Clinical & Medical Case Studies
Copyright: © Bashir BA (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License
Citation: Hassan MM, Bashir BA. Unraveling hematological and coagulation pattern in malaria: A study from Kassala City, Eastern Sudan. Int J Clin Med Case Stud. 2025; 2(1): 1011.
Background: Malaria continues to pose a significant public health concern in Eastern Sudan. This study assesses the hematological parameters and coagulation profile among malaria-infected patients in Kassala City. The disease, caused by Plasmodium parasites and transmitted through the bite of infected Anopheles mosquitoes, leads to significant morbidity and mortality. Malaria infection induces a range of hematological and coagulation abnormalities, including anemia, thrombocytopenia, and alterations in coagulation profiles.
Objectives: This study attempts to discover notable hematological and coagulation alterations linked to malaria and to examine differences among various malaria types, therefore offering insights for enhanced diagnosis and clinical course of the disease.
Materials and methods: This cross-sectional analytical study included 217 participants, 167 malaria-infected patients, and 50 healthy controls. Hematological parameters Hemoglobin (HB), Red cell indices, Red cell Distribution Width (RDW), Platelet Count (PLT), platelet indices, and coagulation profiles (PT, INR, APTT, D-dimer) were measured. Statistical analysis included the Shapiro-Wilk, Mann-Whitney U, and Kruskal-Wallis tests.
Results: Malaria cases showed significantly lower HB (12.328±2.112 vs. 13.022±1.582, P<0.022) and PLT (196.922±102.774 vs. 316.760±96.170, P<0.000) and higher D-dimer levels (399.24±111.8 vs. 0.4442±91.77, P<0.001) compared to controls. Significant variations in RDW (P=0.048), MPV (P=0.012), PT (P=0.012), and PTT (P=0.008) were observed between malaria types.
Conclusion: The principal findings encompass increased D-dimer levels (hyperfibrinolysis) and significant thrombocytopenia, emphasizing the importance of platelet indices as vital indicators of disease severity. Furthermore, inconsistencies in RDW, MPV, PT, and PTT among various malaria types indicate unique effects on hematological parameters that could affect patient care.
Keywords: Platelet indices; Coagulation; Hematological parameters; D-Dimer; Kassala.
Malaria continues to pose a substantial public health concern in numerous areas globally, especially in countries like Eastern Sudan [1]. The ailment, induced by the Plasmodium parasite and conveyed via infected Anopheles mosquitoes’ bite, results in various hematological and coagulation disorders [2]. Recognizing these factors is essential for enhancing malaria diagnosis, treatment, and management and formulating efficient public health initiatives [2,3].
Prior research has demonstrated that malaria infection may lead to anemia, thrombocytopenia, and coagulopathy, complicating the clinical progression of the disease [2]. A study in Northwest Ethiopia revealed that malaria patients demonstrated extended Prothrombin Time (PT), heightened International Normalized Ratio (INR), increased Activated Partial Thromboplastin Time (APTT), and diminished platelet counts [1]. Research in Sudan similarly indicated a high incidence of severe anemia and thrombocytopenia in malaria patients, accompanied by notable changes in PT and D-Dimer [4].
In addition to these findings, malaria infection has been associated with significant platelet and red cell indices changes [5,6]. These implications highlight the pressing necessity for additional research and clinical interventions. Studies have shown that malaria patients often exhibit reduced Mean Platelet Volume (MPV), Plateletcrit (PCT), and Platelet Distribution Width (PDW), along with lower Red Blood Cell (RBC) counts, Hemoglobin (Hb) levels, and Mean Corpuscular Volume (MCV). A critical red cell index, the Red cell Distribution Width (RDW), which measures the variation in the size of red blood cells, has also been observed to increase in malaria patients. Elevated RDW levels can indicate a mix of young and old red blood cells in the bloodstream, reflecting the body’s response to the hemolysis and anemia caused by the malaria infection [5]. The platelet and red cell indices’ modifications can be significant indicators of the severity and advancement of malaria infection [5,6].
This study centered on Kassala City to thoroughly investigate hematological and coagulation alterations in malaria-infected patients. It enhances the overall comprehension of malaria’s effects on blood parameters and coagulation mechanisms. The results may guide clinical practices and public health strategies to alleviate the burden of malaria in the region.
Study design and setting
This cross-sectional analytical study was conducted in Kassala City, Eastern Sudan, from 2021 to 2023. Kassala City is located in eastern Sudan and is known for its high malaria prevalence due to its endemic nature.
Study population and sampling
The study population comprised malaria-infected patients visiting healthcare facilities in Kassala City. It included 217 volunteers, 167 malaria-infected individuals, and 50 healthy control persons. The control group comprised individuals with no prior history of malaria infection, matched by age and gender to the malaria-infected group.
Inclusion and exclusion criteria
The inclusion criteria for malaria-infected individuals were confirmed malaria diagnosis using microscopy and/or Rapid DiDiagnostic Tests (RDTs), age exceeding 18 years, and willingness to participate in the study with informed consent. The exclusion criteria, meticulously designed to ensure the survey’s integrity, included the presence of additional infectious illnesses or comorbidities, pregnant women, individuals on anticoagulant therapy, or those transfused with blood and blood products.
Data collection
A standardized questionnaire gathered data to acquire demographic and clinical information. Venous blood samples (5 mL) were obtained from each subject employing aseptic procedures. The blood samples were partitioned into two segments: hematological analysis (K3EDTA) and coagulation profile evaluation (3.2% Tri-sodium citrate).
Hematological parameters assessment
Hematological parameters, including Red Blood Cell (RBC) count, Hemoglobin (Hb) level, Hematocrit (Hct), Mean Corpuscular Volume (MCV), Mean Corpuscular Hemoglobin (MCH), Mean Corpuscular Hemoglobin Concentration (MCHC), Red cell Distribution Width (RDW), platelet count, Mean Platelet Volume (MPV), Plateletcrit (PCT), and Platelet Distribution Width (PDW), Platelet Large Cell Rratio (PLCR), Platelet Large Cell Concentration (PLCC) were measured using three-part semi-automated hematology analyzer (Mindray B30s, China).
Coagulation profile assessment
The coagulation profile, including Prothrombin Time (PT), International Normalized Ratio (INR), Activated Partial Thromboplastin Time (APTT), and D-Dimer, was assessed using standard laboratory techniques (Coagulometer).
Data analysis
Data were analyzed using statistical software. Descriptive statistics were used to summarize the demographic and clinical characteristics of the study population. The mean and Standard Deviation (SD) were calculated for continuous variables. The Shapiro-Wilk test was employed to assess the normality of the data distribution. The data were not normally distributed, so non-parametric tests were used for further analysis. The Mann-Whitney U test was applied to compare hematological and coagulation parameters between malaria-infected patients and healthy controls. Kruskal-Wallis’s test was used to compare the two groups’ Red cell Distribution Width (RDW). A p-value of <0.05 was considered statistically significant.
Ethical considerations: The research complied with the ethical guidelines set by the institutional review board. All individuals provided informed consent before enrolling in the study, and the confidentiality and identities of the participants were preserved throughout the research process.
A total of 217 blood samples were collected from various regions in Kassala State. 158 samples (72.8%) tested positive for Plasmodium falciparum, 9 samples (4.1%) tested positive for Plasmodium vivax, and 50 samples (23.1%) were malaria-negative, serving as the control group.
Demographic data
Of the 158 P. falciparum-positive cases, 130(59.9%) were from urban areas, while 28 (12.9%) were from rural areas, as detailed in Table 1. This difference was statistically significant (P<0.0001). Among the P. falciparum-positive cases, 81(37.3%) were male, and 77(35.5%) were female. The P. vivax-positive cases and the malaria-negative controls had similar distributions, with a (P<0.102). Out of the 167 cases, 165(76%) exhibited no clinical manifestations of bleeding, while 1 case (0.5%) presented with epistaxis and another (0.5%) with a rash with a (P<0.945). The control group of 50 individuals showed no clinical bleeding manifestations. The ages of the patients ranged from 1 to 80 years, with an insignificant (P<0.159).
Baseline characteristics
The baseline characteristics of malaria cases and control subjects are summarized in Table 1. The mean Hemoglobin (HB) level was significantly lower in malaria cases (12.328±2.112) compared to controls (13.022±1.582), with a (P<0.022). Hematocrit (HCT) values were slightly lower in malaria cases (37.965±7.070) compared to controls (39.090±4.129), but this difference was not statistically significant (P=0.330). Similarly, Red Blood Cell (RBC) counts, Mean Corpuscular Volume (MCV), Mean Corpuscular Hemoglobin (MCH), and Mean Corpuscular Hemoglobin Concentration (MCHC) showed no significant differences between the two groups.
However, Platelet Count (PLT), Plateletcrit (PCT), and Platelet Large Cell Ratio (PLCR) were significantly lower in malaria cases compared to controls, with (P<0.000) for each parameter. The groups’ Mean Platelet Volume (MPV) and Platelet Distribution Width (PDW) were similar. Total White Blood Cell (WBC) count was not significantly different between malaria cases (5.981±2.396) and controls (6.236±1.508). Notably, neutrophil counts were higher in malaria cases (63.210±14.484) than in controls (55.176±11.565), with a (P<0.000). In comparison, lymphocyte counts were lower in malaria cases (26.275±12.908) compared to controls (35.100±11.035), with a (P<0.000). Monocyte counts and eosinophil counts showed no significant differences between the groups, although eosinophils were slightly higher in malaria cases (3.026±2.886) compared to controls (1.928±1.853), with a p-value of 0.037. Basophil counts were similar in both groups.
Coagulation profile
The coagulation profile revealed that Prothrombin Time (PT) was significantly prolonged in malaria cases (14.815±4.133) compared to controls (13.566±1.497), with a (P<0.006). The International Normalized Ratio (INR) was slightly higher in malaria cases (1.1163±0.401) compared to controls (1.0962±0.231), but this difference was not statistically significant (P=0.840). The activated Partial Thromboplastin Time (PTT) was significantly shorter in malaria cases (37.078±6.993) compared to controls (38.598±44.28), with a (P<0.000). D-dimer levels were notably higher in malaria cases (399.24±111.8) than in controls (0.4442±91.77), with a (P<0.001).
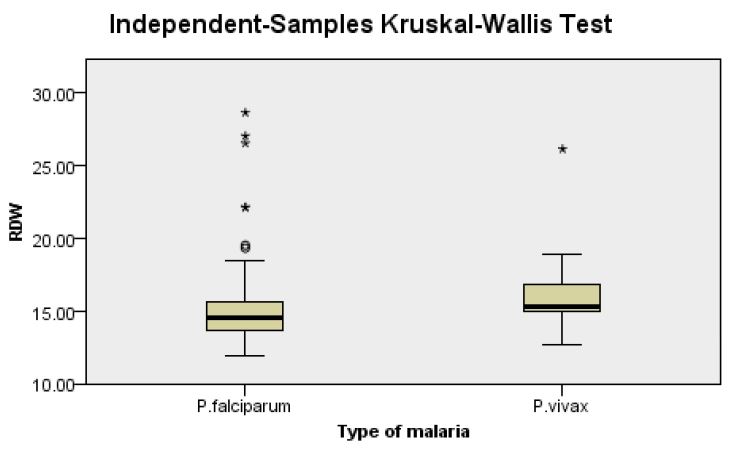
Our findings indicate notable disparities between malaria types and specific blood parameters, such as RDW (P=0.048): RDW exhibits notable discrepancies, indicating variances in the distribution of red blood cell sizes among different malaria types (Figure 1). MPV (P=0.012): Mean Platelet Volume (MPV) levels exhibit significant variation, reflecting alterations in platelet size according to the malaria type. PT (P=0.012): Prothrombin Time (PT) demonstrates significant variances, indicating variability in the blood coagulation mechanism between distinct malaria types. PTT (P=0.008): PTT demonstrates significant variations, underscoring the influence on coagulation processes attributattributable to distinct malaria types. D-Dimer (P=0.036): Significant differences in D-Dimer levels indicate changes in fibrinolysis and the degradation of blood clots contingent upon the type of malaria.
| Variables | Malaria cases (n=167) Mean±SD | Control(n=50) Mean±SD | P.value |
|---|---|---|---|
| HB | 12.328±2.112 | 13.022±1.582 | 0.022 |
| HCT | 37.965±7.070 | 39.090±4.129 | 0.330 |
| RBC | 4.493±0.649 | 4.588±0.422 | 0.248 |
| MCV | 85.061±8.660 | 85.198±7.444 | 0.854 |
| MCH | 27.315±3.697 | 27.900±2.632 | 0.207 |
| MCHC | 32.450±2.936 | 32.908±2.861 | 0.227 |
| RDW-CV | 15.065±2.515 | 14.464±2.369 | 0.143 |
| PLT | 196.922±102.774 | 316.760±96.170 | 0.000 |
| PCT | 0.1673±0.09907 | 0.2462±0.0660 | 0.000 |
| PLCR | 19.580±4.830 | 22.572±4.3806 | 0.000 |
| PDW | 15.629±1.363 | 15.466±0.7195 | 0.086 |
| PLCC | 196.922±102.774 | 316.760±96.170 | 0.000 |
| WBC | 5.981±2.396 | 6.236±1.508 | 0.830 |
| Neutrophils | 63.210±14.484 | 55.176±11.565 | 0.000 |
| Lymphocytes | 26.275±12.908 | 35.100±11.035 | 0.000 |
| Monocytes | 7.416±2.536 | 7.144±1.814 | 0.650 |
| Eosinophils | 3.026±2.886 | 1.928±1.853 | 0.037 |
| Basophils | 0.01±0.077 | 0.00±0.000 | 0.584 |
| PT | 14.815±4.133 | 13.566±1.497 | 0.006 |
| INR | 1.1163±0.401 | 1.0962±0.231 | 0.840 |
| PTT | 37.078±6.993 | 38.598±44.28 | 0.000 |
| D-Dimer | 399.24±111.8 | 0.4442±91.77 | 0.001 |
This study’s findings reveal substantial hematological and coagulation alterations in malaria-infected patients relative to healthy controls in Kassala City, Eastern Sudan. The diminished HB levels and elevated D-dimer levels in malaria cases align with prior research demonstrating anemia and heightened fibrinolysis in infected individuals [1,3]. The notable decrease in PLT and PCT in malaria cases corresponds with the established occurrence of thrombocytopenia in malaria infections [3]. Studies have shown that lower PLT, MPV, and PDW levels indicate more severe malaria infections and can be used to monitor treatment efficacy and predict disease progression [7].
and PCT in malaria cases corresponds with the established occurrence of thrombocytopenia in malaria infections [3]. Studies have shown that lower PLT, MPV, and PDW levels indicate more severe malaria infections and can be used to monitor treatment efficacy and predict disease progression [7].
Our data reveal significant differences between malaria forms and particular blood parameters. RDW demonstrated notable differences (P=0.048), signifying variations in the distribution of red blood cell sizes among several malaria types [11]. MPV levels exhibited substantial variation (P=0.012), indicating changes in platelet size based on the kind of malaria [12]. PT exhibited substantial differences (P=0.012), reflecting diversity in the blood coagulation process among different malaria types [13]. PTT exhibited notable variability (P=0.008), highlighting the impact of different malaria types on coagulation processes [14]. Moreover, notable variations in D-dimer levels (P=0.036) suggest alterations in fibrinolysis and the breakdown of blood clots dependent on the malaria type [15]. The data indicate that several malaria types may uniquely affect hematological and coagulation parameters, impacting patient management and treatment techniques.
Interestingly, the extended PT and shortened PTT noted in malaria cases indicate a complicated modification in the coagulation cascade, likely engaging both pro-coagulant and anticoagulant pathways [16]. Research indicates that Plasmodium falciparum-infected red blood cells can stimulate tissue factor expression in endothelial cells, resulting in thrombin production and a prothrombotic condition [16,17].
Increased D-dimer levels have been recognized as a possible biomarker for malaria infections, indicating extreme severity and hypercoagulability. A systematic review and meta-analysis by Sukati et al. (2024) [18] demonstrated notable increases in D-dimer levels in individuals infected with Plasmodium, especially those with malaria. The elevated levels signify enhanced fibrinolysis and possible thrombotic consequences, rendering D-dimer a significant marker for evaluating disease risk and development. The clinical progression of malaria may vary from moderate to severe, with potential complications including cerebral malaria, severe anemia, and multi-organ failure. Increased D-dimer levels may assist in identifying individuals at heightened risk of severe consequences, facilitating prompt interventions and enhancing patient outcomes. Further study is necessary to standardize D-dimer measurement techniques and establish its clinical use in malaria care [19].
This study’s strength is its thorough evaluation of many hematological and coagulation markers, offering an in-depth understanding of malaria’s effects on these factors. The incorporation of a control group and the application of non-parametric tests to address non-normally distributed data enhance the robustness of the findings. The study’s emphasis on both Plasmodium falciparum and Plasmodium vivax infections facilitates a more detailed examination of the distinctions between malaria forms.
Nevertheless, the study possesses certain drawbacks. The cross-sectional design restricts the capacity to deduce causality and evaluate temporal changes. The sample size, especially for Plasmodium vivax patients, was comparatively limited, potentially impacting the generalizability of the results. Moreover, the study utilized blood samples from a singular geographic area, and the results may not accurately reflect other places exhibiting distinct epidemiological patterns of malaria. Future research should incorporate longitudinal studies utilizing larger sample sizes and diverse locales to corroborate and expand upon these findings.
This study reveals significant hematological and coagulation changes in malaria-infected patients in Kassala City, Eastern Sudan. The key findings include elevated D-dimer levels, hyperfibrinolysis, and significant thrombocytopenia, highlighting the role of platelet indices as crucial markers for disease severity. Additionally, variations in RDW, MPV, PT, and PTT between different malaria types suggest distinct impacts on hematological parameters that may influence patient management.