-
Email info@ijcmcs.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
11Internal Medicine, Hospital Universitario De Torrejón, Spain.
2Medical Student, Ghent University, Belgium.
3Medical Oncology, Hospital Universitario De Torrejón, Spain.
4Department of Pharmacy and Nutrition, Faculty of Biomedical and Health Sciences, Universidad Europea de Madrid, Spain.
5Universidad Francisco de Vitoria, Spain.
*Corresponding author: Luis Cabezón-Gutiérrez
GutiérrezMedical Oncology, Torrejón University Hospital, Calle Mateo Inurria Nº1. Madrid, Spain.
Faculty of Medicine, Francisco de Vitoria University, Ctra, Pozuelo-Majadahonda KM 1.800. 28223 Pozuelo de Alarcón Madrid, Spain.
Email: pitucgp@hotmail.com
Received: Mar 28, 2025
Accepted: Apr 16, 2025
Published Online: Apr 23, 2025
Journal: International Journal of Clinical & Medical Case Studies
Copyright: © Cabezón-Gutiérrez L (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License
Citation: Gallego-Nieto S, Avdic S, Pacheco-Barcia V, Custodio-Cabello S, Cabezon-Gutierrez L, et al. Hypersensitivity reaction to selpercatinib in a patient with RET fusion-positive lung adenocarcinoma and testicular metastasis. Int J Clin Med Case Stud. 2025; 2(1): 1018.
Non-Small Cell Lung Cancer (NSCLC) frequently harbors actionable genetic alterations, including RET fusions, which occur in 1–2% of cases, predominantly in adenocarcinomas. Selpercatinib, a selective RET inhibitor, has significantly improved outcomes in these patients, demonstrating high response rates even following prior therapies. However, testicular metastases from lung adenocarcinoma are exceedingly rare, likely due to the protective blood testis barrier and lower scrotal temperatures. Similarly, uncommon are hypersensitivity reactions to selpercatinib, particularly in patients with prior exposure to immune checkpoint inhibitors (ICIs), which may increase susceptibility. Here, we present a unique case that com-bines these rare phenomena, offering insight into their clinical interplay.
Keywords: Lung adenocarcinoma; Selpercatinib; Testicular metastasis; RET fusion.
Lung carcinoma remains one of the most aggressive malignancies worldwide, frequently presenting with distant metastases at the time of diagnosis. While common metastatic sites include the brain, liver, adrenal glands, and bones, testicular metastasis from lung carcinoma is an exceedingly rare occurrence, with an estimated incidence ranging from 0.06% to 0.46% in autopsy studies [1]. This rarity may be attributed to the unique microenvironment of the testes, including the low scrotal temperature and the blood-testis barrier, which is thought to limit the hematogenous spread of malignant cells [2].
Despite its infrequent occurrence, testicular metastasis from lung cancer presents a diagnostic and clinical challenge. Often, these secondary tumors mimic primary testicular neoplasms, complicating the differential diagnosis [3]. Histologically, lung adenocarcinoma with metastasis to the testis can exhibit glandular structures with mucinous differentiation, while squamous cell carcinoma metastases may present as solid nests with keratinization [1]. Immunohistochemical analysis, including Thyroid Transcription Factor-1 (TTF-1) and cytokeratin profiling, plays a critical role in distinguishing these metastatic lesions from primary testicular tumors [2].
Clinically, testicular metastases may present as painless testicular masses, often discovered incidentally during staging investigations or follow-up imaging [3]. However, in some cases, they remain asymptomatic until autopsy. The mechanism of testicular metastasis is still not fully clarified, though hematogenous dissemination appears to be the primary route, given the vascular nature of lung carcinoma [4]. Other proposed pathways include retrograde lymphatic spread or direct extension in cases with extensive pelvic involvement [2].
The presence of testicular metastasis in lung carcinoma patients often indicates advanced disease and a poor prognosis. Systemic chemotherapy remains the cornerstone of treatment, though testicular metastases have been reported to exhibit resistance due to the blood-testis barrier [5]. Emerging treatment approaches, such as Immune Checkpoint Inhibitors (ICIs) targeting Programmed Death-Ligand 1 (PD-L1), have demonstrated promising results in select cases [6].
The clinical case presented below concerns a patient with lung adenocarcinoma harboring a RET fusion, who initially manifested with a testicular mass and subsequently developed a hypersensitivity syndrome to RET inhibitors following first-line chemo-immunotherapy. This case will review the pathophysiology, diagnostic challenges, and treatment approaches associated with testicular metastases originating from lung carcinoma, as well as the management of hypersensitivity syndrome to RET inhibitors post-immunotherapy. Through an analysis of existing literature and case reports, the authors aim to provide insights into this rare but significant manifestation of metastatic lung cancer, being the only published case to date of testicular metastasis in lung adenocarcinoma with RET fusion.
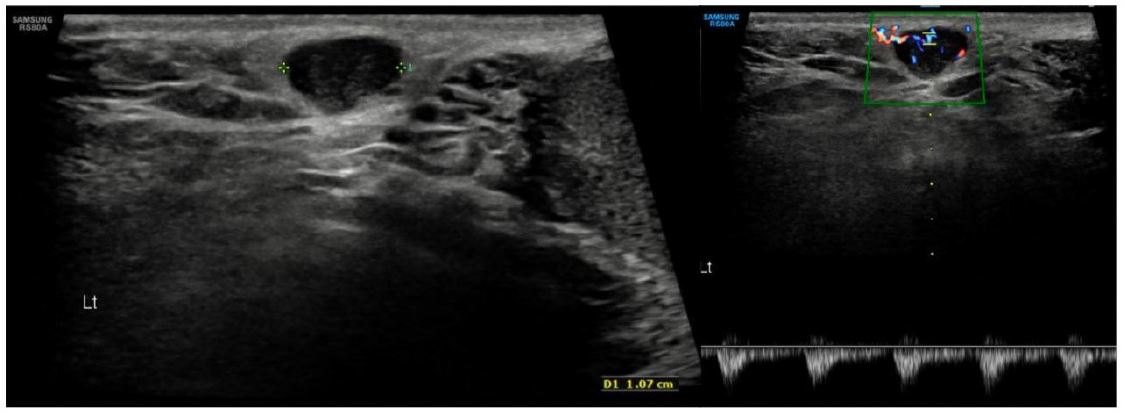
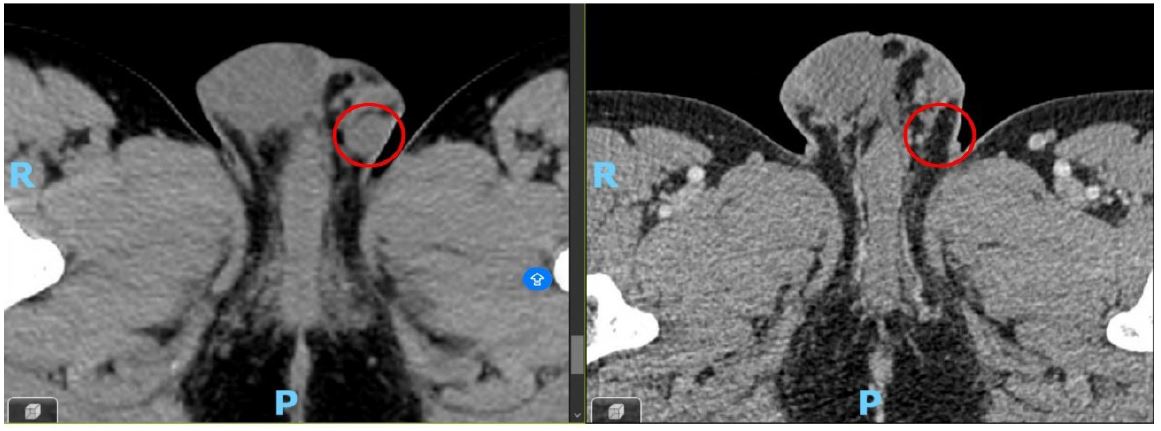
A 45-year-old male, former smoker (2 package index year) with no significant medical history, presented to Internal Medicine in May 2023 with a 4-month history of persistent dry cough and pleuritic chest pain. A chest X-ray revealed an opacity in the right lower lobe, initially of uncertain inflammatory or infectious etiology. The patient also reported a left scrotal lesion, noticed months earlier, presumed to be a lipoma and awaiting excision. A left testicular ultrasound was performed, revealing an oval-shaped lesion measuring approximately 11×5 mm (Figure 1).
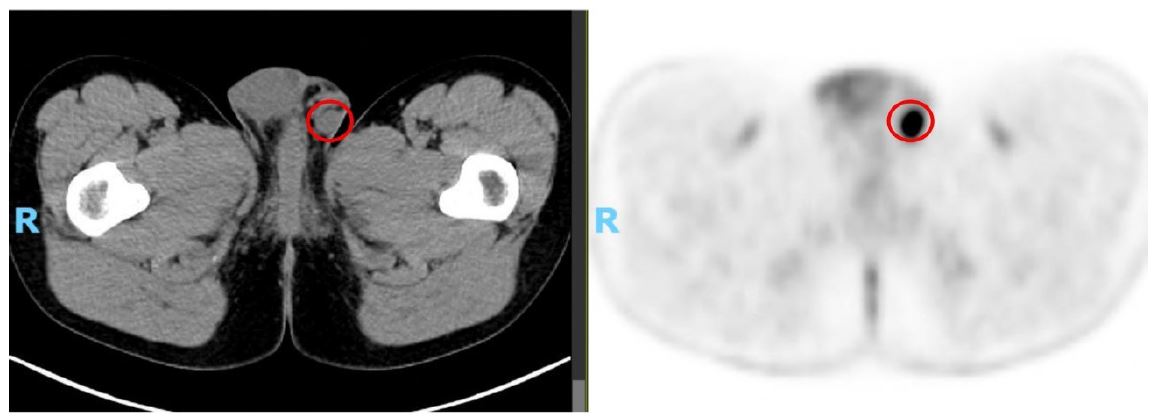
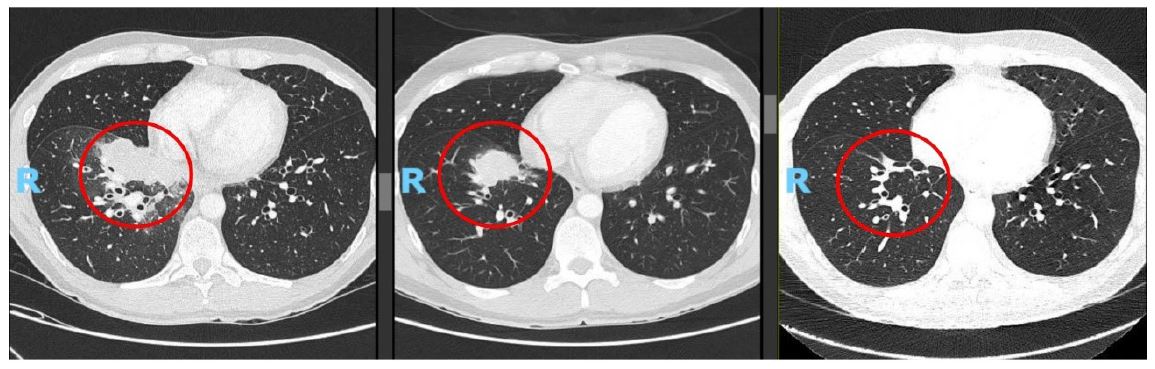
Given persistent respiratory symptoms without evidence of infection, a chest Computed Tomography (CT) scan was conducted, revealing a solid lesion in the right lower lobe suggestive of a primary tumor, accompanied by bilateral hilar lymphadenopathies. Subsequent Positron Emission Tomography-Computed Tomography (PET)-CT demonstrated elevated metabolic activity in the pulmonary lesion, bilateral hilar, cervical, mediastinal, and left inguinal lymphadenopathies, and a probable metastatic left scrotal lymph node (Figure 2).
Bronchoscopy revealed bronchial inflammation and partial occlusion of the middle lobe, with no evident endobronchial lesions; biopsy confirmed poorly differentiated adenocarcinoma. Molecular profiling showed no alterations in EGFR, ALK, or ROS1, while PD-L1 expression was 95%. Next-generation sequencing detected a KIF5B(15)–RET(12) fusion. Biopsy of the scrotal lesion confirmed metastatic adenocarcinoma of pulmonary origin.
In June 2023, first-line chemo-immunotherapy (carboplatin AUC 5 plus pemetrexed 500 mg/m2 plus pembrolizumab 200 mg iv every 21 days for four cycles) was initiated, achieving a partial response, followed by maintenance therapy with pemetrexed plus pembrolizumab at the same dose. Disease progression was observed after 8 months, leading to second-line treatment with selpercatinib (RET inhibitor) in February 2024.
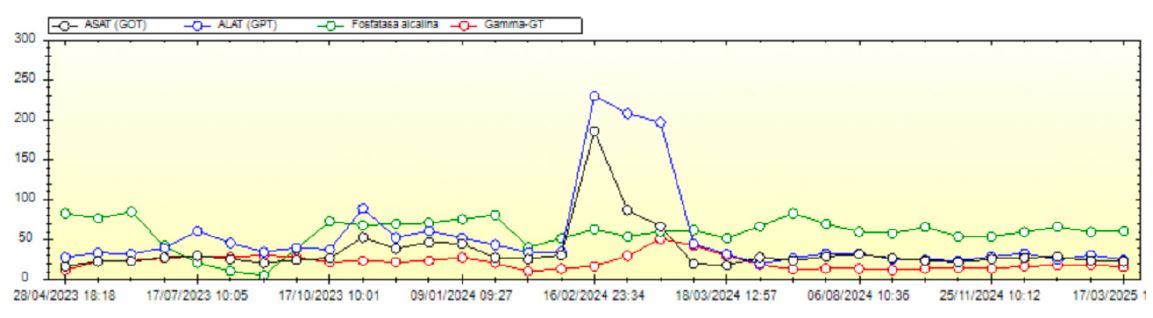
One week after initiating selpercatinib, the patient developed fever of unknown origin, prompting empirical levofloxacin therapy. Within 24 hours, a generalized erythematous rash (sparing palms and soles) appeared. Admitted for suspected toxicoderma (levofloxacin vs. selpercatinib), he presented with febrile neutropenia, thrombocytopenia, and elevated transaminases (Figure 3). Treatment with corticosteroids and antihistamines resolved the rash and fever within four days. Selpercatinib was reintroduced 36 hours after fever resolution during hospitalization, but fever recurred, indicating a probable hypersensitivity reaction.
One week following discharge, while receiving corticosteroids, selpercatinib was reintroduced at half the standard dose with excellent tolerability, subsequently escalating to the full dose two months later without adverse events. Thereafter, the only notable side effects were edema-related weight gain, necessitating furosemide initiation with stabilization after 4-5 months, and self-limiting abdominal pain without diarrhea or concerning features, which resolved spontaneously.
At the first reassessment after four cycles of selpercatinib, a response was observed, marked by a significant reduction in tumor mass and disease stability confirmed by subsequent imaging (Figures 4 & 5).
After 14 cycles of selpercatinib, the patient exhibits sustained disease stability and treatment response, with favorable tolerability and maintained quality of life.
Non-Small Cell Lung Cancer (NSCLC), particularly adenocarcinoma, predominates among nonsmokers or those with minimal smoking history, as exemplified by our patient. In younger patients, this subtype is frequently associated with actionable genetic alterations, requiring comprehensive molecular profiling. Beyond PD-L1 assessment for immunotherapy, evaluating EGFR, ALK, ROS1, and performing Next-Generation Sequencing (NGS) are critical, as demonstrated by the identification of a KIF5B(15)–RET(12) fusion in our case [7].
RET fusions occur in 10–20% of papillary thyroid cancers and 1–2% of NSCLC, predominantly adenocarcinomas [8]. Selpercatinib, a selective RET inhibitor, is approved as first- or second-line therapy for RET fusion-positive tumors, demonstrating efficacy in this population. In the LIBRETTO-001 phase I/II trial, treatment-naïve patients achieved a 6% complete response rate, with 40% ongoing responses, overall responses were observed in 64% of patients with selpercatinib (compared with a response rate of 15% to the last prior therapy received before enrollment, P=0.001) and median Progression-Free Survival (PFS) was of 22 months. In pretreated patients, showed a 7% complete response rate, 49% ongoing responses, and a median PFS of 24.9 months [9]. These findings are consistent with our patient’s PFS of at least 13 months on second-line selpercatinib.
Despite its efficacy, selpercatinib safety profile includes notable adverse events, with hypersensitivity reactions reported in 7% of LIBRETTO-001 participants, primarily grade 1–2, occurring a median of 1.7 weeks post-initiation [9]. These reactions manifest as fever, rash, generalized edema, hepatic dysfunction, renal impairment, and thrombocytopenia—consistent with our patient’s presentation of fever, rash, thrombocytopenia, and elevated transaminases 7–8 days after starting selpercatinib. Prior chemo-immunotherapy, as in our case (carboplatin, pemetrexed, pembrolizumab), increases this risk. The SIREN study reported a 100% incidence of adverse effects in immunotherapy-pretreated patients versus 80% in treatment-naïve patients [8], while LIBRETTO-001 noted rates of 77% versus 23%, respectively [9].
Data from LIBRETTO-001 suggest that hypersensitivity reactions to selpercatinib do not necessitate permanent discontinuation; among 22 affected patients, only two discontinued treatments following the initial reaction, and one ceased after recurrence upon rechallenge, whereas 19 successfully resumed selpercatinib with concurrent corticosteroid support, avoiding severe recurrence, although not all achieved the full dose [9].
The recommended hipersensibility management includes: withholding selpercatinib until resolution of the event, initiating prednisone at 1 mg/kg daily or an equivalent corticosteroid, providing Pneumocystis prophylaxis and gastric protection, and conducting a physical examination (including skin assessment) alongside laboratory evaluations (CBC with differential, CMP, IL-6, and CRP). Upon resolution, resume selpercatinib at a dose reduced by three levels from that administered prior to the onset of hypersensitivity. Incrementally increase the dose weekly by one level, as tolerated, until reaching the pre-hypersensitivity dose. Maintain corticosteroid therapy until the target dose is achieved, followed by a gradual taper [5].
In our patient, suspected selpercatinib-induced hypersensitivity led to drug withdrawal and initiation of corticosteroids. Following management guidelines, selpercatinib was reintroduced at a reduced dose after symptom resolution, alongside corticosteroids, reaching the full dose within two months. Subsequent mild adverse effects, including edema (controlled with furosemide) and self-limiting abdominal pain, are consistent with established tolerability profiles.
A distinctive feature of this case is the confirmed left testicular metastasis. Testicular metastases are rare, comprising 3.6% of testicular tumors, with their infrequency potentially attributable to lower scrotal temperatures or the blood-testis barrier [3,10]. Most are identified posthumously or during orchiectomy for metastatic prostate cancer [2,4]. Non-incidental presentations are uncommon, requiring differentiation from primary testicular tumors (>90% of cases) [1]. In a review of 26 non-incidental testicular metastases, only 38% had a known primary tumor, predominantly prostate, with unilateral involvement typical [2]. Excluding lymphomas and leukemias, prostate and lung cancers most commonly metastasize to the testes, the latter via hematogenous spread [11]. While lung adenocarcinoma with testicular metastases is documented, no prior reports describe RET fusion-positive cases, rendering this presentation unique.
This case highlights the rare occurrence of testicular metastasis in RET fusion-positive lung adenocarcinoma and a hypersensitivity reaction to selpercatinib following prior chemo-immunotherapy. The patient achieved a sustained response with a PFS of at least 13 months on second-line selpercatinib, despite initial hypersensitivity managed successfully with initial dose reduction and corticosteroids. These findings underscore the importance of molecular profiling in NSCLC and the feasibility of managing selpercatinib-related adverse events, offering insights into its tolerability and efficacy in complex clinical scenarios.
Conflicts of interest: Luis Cabezón-Gutiérrez reports he received payment for presentations of Roche, Astra Zeneca, Brystol Myers Squibb, Merck Serono, Ipsen Pharma, Grunenthal, Kyowa Kirin, Pfizer and Eisai and received support for attending meetings from Roche, Merck. Eli Lilly, Bristol-Myers Squibb and Nutricia. Vilma Pacheco Barcia reports she received a grant as an award from Merck and FSEOM and grant from Pfizer. Payment for presentations of Merck, Eli Lilly, Eisai and Pierre Fabre and received support for attending meetings from Roche, Eli Lilly, Bristol-Myers Squibb, Merck, Amgen, Merck Sharp and Dhome, and Nutricia. Vilma Pacheco Barcia also reports she participated in an advisory board from advanced accelerator applications, a Novartis company and Nutricia. Sara Custodio-Cabello has received honoraria (outside of this submitted study) from Fresenius, Astellas Pharma, Merck and Abbott and received support for attending meetings from Pierre-Fabre and Amgen. Magda Palka-Kotlowska has received payment for presentations of Pfizer, Devon, Pharmamar, and Esteve and received support for attending meetings from Pfizer and Novartis. Sheherezade Gallego-Nieto, José Ramón Sevilla-Resúa, Selma Avdic and Beatriz Chacón-Ovejero, have no conflicts of interest to declare. All the authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval: No ethical approval was required for this article
Informed consent: Written informed consent was obtained from the patient for the anonymized information to be published in this article.