-
Email info@ijcmcs.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Clinical Professor and Past Chair of Oral & Maxillofacial Pathology, Department of Oral & Maxillofacial Surgery, West Virginia University, Morgantown, West Virginia.
2Associate Professor and Director of Oral & Maxillofacial Radiology, Department of Oral & Maxillofacial Surgery, West Virginia University, Morgantown, West Virginia
3Assistant Professor & Director of Biopsy Service, Department of Oral & Maxillofacial Surgery, West Virginia University, Morgantown, West Virginia.
*Corresponding author: Jerry E Bouquot
Clinical Professor and Past Chair of Oral & Maxillofacial Pathology, Department of Oral & Maxillofacial Surgery, West Virginia University, 212 Tibbs Road, Morgantown 26508, West Virginia.
Email ID: bouquot@aol.com
Tel: 281-745-2330
Received: Apr 14, 2025
Accepted: Apr 29, 2025
Published Online: May 05, 2025
Journal: International Journal of Clinical & Medical Case Studies
Copyright: © Bouquot JE (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License
Citation: Bouquot JE, Garladinne L, Luna M. Ameloblastic carcinoma - malignant variant of a most unusual odontogenic tumor. Int J Clin Med Case Stud. 2025; 2(1): 1020.
The ameloblastoma, first reported as an “odontome” in 1827, has long been known as one of the most unusual and complex of odontogenic tumors, with a variety of clinical and microscopic types (Table 1) [1,2]. By 1928 it became clear that this benign, locally aggressive neoplasm with its large growth potential had an additional unique feature: it occasionally formed distant metastases from lesions with exactly the same benign, nondysplastic odontogenic epithelium as a “normal” ameloblastoma; even the metastatic foci looked benign [3-5]. Such lesions, now known as Malignant Ameloblastomas or Metastasizing Ameloblastomas (METAM), most often spread to the lungs where they provide yet another diagnostic challenge: they must be distinguished from aspiration ameloblastomas, produced when cells from the original jaw lesion are aspirated during surgical removal [7]. Aspirated lesional cells are able to implant into bronchiole walls and proliferate into a noticeable tumor,
So, the biological behavior of microscopically benign ameloblastomas has been puzzling, but there also is a truly and obviously malignant variant of the lesion: the Ameloblastic Carcinoma (AC) [8-10]. This shows variable levels of cellular dysplasia and behaves like most other local malignancies, including the ability to dramatically destroy normal tissues locally and to metastasize to all parts of the body. We present herein a case report of ameloblastic carcinoma.
Keywords: Ameloblastic carcinoma; Ameloblastoma; Malignant ameloblastoma; Metastatic ameloblastoma; Odontogenic tumors; Malignant odontogenic tumors.
Clinical presentation
A 68-year-old female presented to her dentist for evaluation of an asymptomatic “big bulge” of her right maxilla (Figure 1). She first noticed it 5 months earlier and claimed that it had continuously enlarged since that time. At examination there was a large, sessile, smooth-surfaced mass which was firm to palpation. The expansion extended from the right lateral incisor area to the long-edentulous molar region and was virtually all toward the facial, with minimal elevation of the crestal region of the alveolus. The surface mucosa was unremarkable and there were no other masses present, except for a small, lobulated torus palatinus. No neckmass could be detected.
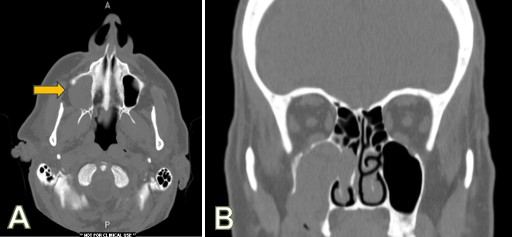
Radiology
CT imaging showed that the expansile mass consisted of soft tissue which had destroyed the facial cortex of the right maxillary alveolus, destroyed the right maxillary sinus bony floor and lateral wall, and completely filled the sinus. It also had perforated through the medial wall of the sinus to fill much of the right nasal sinus, extending superiorly into the ethmoid region (Figure 2). The infraorbital bone at the top of the maxillary sinus also appeared to be partially destroyed.
Histopathology
Incisional biopsy was performed. Microscopically, the mass was comprised of large and small islands of mildly to moderately dysplastic cuboidal and oval epithelial cells with large nuclei, sometimes with gland-like features, sometimes with plexiform trabeculations and sometimes with areas showing polarization of columnar peripheral cells, all within an uninflamed background stroma of dense fibrous tissue (Figures 3 & 4). When in contact with adjacent or surrounding bone lesional cells were destroying the bone and proliferating into the resulting bone loss areas: remaining bone appeared viable and mature. The great majority of the large islands of lesional epithelial cells had no duct-like structures and had peripheral cells identical to the preameloblasts surrounding epithelial islands in ameloblastomas (Figures 4A-4C). A few areas also contained epithelial islands with features of classic ameloblastoma (Figure 4D). A diagnosis of ameloblastic carcinoma was made.
Follow-up
Once the diagnosis was made, the patient underwent a bone scan (technetium-99 MDP) and full-body MRI scan, both of which proved negative for metastatic extragnathic lesios. The tumor was then removed via hemimaxillectomy, including removal of the right eye, the turbinates of the right and left nostrils and the entire ethmoid bone. No invasion of the skull base was seen. A maxillofacial prosthesis was made to replace her missing facial components, and she was followed for 3.5 years, during which time there was no evidence of recurrence or metastasis.
| Major Type | Subtype | |
|---|---|---|
| Ameloblastoma | Follicular | |
| Acanthomatous | ||
| Granular cell | ||
| Basal cell | ||
| Keratopapillary | ||
| Desmoplastic | ||
| Unicystic ameloblastoma | ||
| Peripheral (extraosseous) ameloblastoma | ||
| Metastasizing ameloblastoma | ||
| Ameloblastic carcinoma | ||
| Aspiration ameloblastoma |

AC is rare but does account for approximately 2% of odontogenic tumours submitted to oral pathology biopsy services, and it is the most common of odontogenic malignancies, representing approximately 30% of such lesions [7,9,10]. As with so many other malignancies, AC has a varied biological behavior. Overall, 5-year survival is 69%, with some metastases developing up to a decade after initial jaw surgery [10]. Most metastases spread to the lungs and regional lymph nodes, with occasional lesions spreading to the liver, brain and bones. Local recurrence can also be a major issue, especially for maxillary lesions, with one patient developing 8 recurrences over 4 decades [9].
Predicting AC behavior is difficult, as it is with so many H&N malignancies. The more solid tumors, like the present one, typically present a more aggressive radiographic appearance and clinical course, with extensive local destruction of surrounding cortical and adjacent cancellous bone. Less aggressive lesions tend to present with a cystic or multicystic component, with cortical expansion rather than cortical destruction and with radiographic borders that show sclerotic features suggesting that the bone has had a chance to respond to the less aggressive outward growth of the tumor [12]. Overall, almost 47% of ACs present with such well-demarcated borders [12].
The more aggressive lesions, of course, are more likely to present with cervical or more distant metastases at the time of diagnosis, and patients with these have a lower life expectancy, but overall only 10-15% of patients show metastases at diagnosis [12]. Tumor size is also prognostically important, especially for the posterior mandible lesions (85-90% of total), where they generally are 2-9 cm in greatest diameter, The less common maxillary lesions, as with the present case, have more irregular invasion patterns and may even invade the skull base by the time of diagnosis. Behavior and prognosis of maxillary lesions, accordingly, are harder to predict and tend to have higher recurrence and metastasis rates [8,9,11].
Histopathology can also provide prognostic information. More atypical or dysplastic tumor cells tend to predict more aggressive behavior, especially when combined with an increased level of mitotic activity. The present case had minimal numbers of mitoses, perhaps helping to explain its lack of metastases and its uneventful follow-up. Immunohistochemistry thus far has proven to be inconsistently predictable for prognosis, although it appears that the presence of a high level of BRAF-V600E mutations may be an acceptable indicator of aggressive behavior [12,13].
Cases almost always arise de novo, presumably from intramedullary embryonic rests (hamartomas) of odontogenic epithelium within medullary spaces (Figure 5), but occasional cases have arisen, or “transformed,” from benign odontogenic tumors or cysts, including ameloblastomas [8,12]. Conversely, AC may contain regions of benign-appearing ameloblastoma, as seen in Figure 4D.
The microscopic differences between benign ameloblastoma and AC are the same as those seen in almost all other neoplastic types. Lesional cells are more primitive, show a lack of differentiation, are more cellular, have larger, darker and more irregularly shaped nuclei, in addition to a higher rate of mitotic activity. The present example demonstrated all of these except a high rate of mitosis, and it also lacked evidence of another sign of malignancy, vascular and/or perineural invasion. It should be mentioned here that histopathologic variants of AC can make the diagnosis very difficult. These variants include clear cell AC and spindle cell AC [10]. In such cases, immunohistochemistry can aid in confirming a specific diagnosis. The epithelial and spindle cells are positive for cytokeratin, including cytokeratin 19, D2-40, and transducin-like enhancer of split proteins-1 immunohistochemical stains, while the Ki-67 IHC proliferation marker is especially helpful in distinguishing AC from ameloblastoma [10,13].
We present a large ameloblastic carcinoma with direct invasion into the maxillary, nasal and ethmoid sinuses, with perforation of the facial alveolar cortex and soft tissue extension into extracortical tissues. Although extensive and destructive, no metastases were found at the time of diagnosis and none developed during follow-up.