-
Email info@ijcmcs.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Department of Biochemistry, Microbiology, Immunology, Wayne State University School of Medicine, Detroit, USA.
2CS Mott Center for Human Growth and Development, Wayne State University School of Medicine, Department of Obstetrics and Gynecology, Detroit, USA.
3ACA Advanced IVF, Mumbai, India.
*Corresponding author: Savni Sawant
Department of Biochemistry, Microbiology, Immunology, Wayne State University School of Medicine, Detroit, USA.
Email ID: savnisawant@gmail.com
Tel: +1-248-893-5232
Received: May 10, 2025
Accepted: May 27, 2025
Published Online: Jun 02, 2025
Journal: International Journal of Clinical & Medical Case Studies
Copyright: © Sawant S (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License
Citation: Sawant S, Choudhary A. Successful live birth with cryopreserved sperm in a severe oligoasthenoteratozoospermia (OAT) patient using PVP-channel sperm selection technique. Int J Clin Med Case Stud. 2025; 2(1): 1022.
In patients with severe OAT, sperm selection for Intracytoplasmic Sperm Injection (ICSI) poses a significant challenge due to extremely low sperm count, poor motility, and high levels of morphological abnormalities. We report a case where a previously validated microfluidics-inspired Polyvinylpyrrolidone (PVP) channel technique was successfully used to isolate viable sperm from a thawed ejaculate of a severely OAT patient undergoing donor egg IVF. Despite limitations in semen quality and financial constraints prohibiting surgical retrieval options, the adapted PVP technique enabled successful sperm selection, leading to fertilization, blastocyst formation, and a live birth. This report emphasizes the potential of lab-based micromanipulation strategies in overcoming male factor infertility in low-resource IVF settings.
Keywords: Severe OAT; Cryopreserved ejaculate; ICSI; Sperm selection; Microfluidics-inspired technique; Embryo development.
Abbreviations: OAT: Oligoaesthenoteratozoospermia.
OAT is characterized by three hallmark features: a sperm concentration less than 15 million/mL, progressive motility less than 32%, and morphologically normal sperm less than 4%, as per WHO guidelines [3,6,7]. Severe OAT presents additional difficulties, particularly when sperm concentration drops below 1 million/mL and motility is either severely compromised or absent. Traditional semen preparation techniques such as swim-up and density gradient centrifugation rely on the ability of motile sperm to swim through layers of media. In severely compromised samples, these methods often result in excessive sperm loss and enrichment of debris, rendering them ineffective.
When faced with a donor egg cycle, synchronizing sperm availability with oocyte retrieval becomes imperative. Cryopreservation of ejaculate prior to the cycle is often the only viable option for patients who cannot afford to travel to far away clinics often, or opt for surgical sperm retrieval methods such as Testicular Sperm Extraction (TESE) or Percutaneous Epididymal Sperm Aspiration (PESA). However, post-thaw sperm motility can be further diminished due to freeze-thaw injury [1], making sperm retrieval for ICSI from a frozen sample nearly impossible without specialized micromanipulation.
In this report, we present a case at an IVF clinic in Mumbai where a previously published technique using horizontal channels drawn through a viscous PVP streak was utilized to isolate twitching or closest to morphologically normal sperm for ICSI [5]. This method is based on microfluidic principles and allows for visual sorting of sperm that are otherwise hidden in a matrix of cellular debris.
A 45-year-old male partner of a 41-year-old female undergoing donor oocyte IVF presented with severe male factor infertility. The couple had a low socioeconomic background and could not afford genetic testing, repeated ART cycles, or surgical sperm retrieval. As they lived in a rural part of India, they could only afford to come to the clinic a total of two of times; (i) semen freezing during initial consultation and (ii) embryo transfer, and thus could not travel to provide a fresh semen sample on the day of donor oocyte retrieval. Initial semen analysis revealed a sperm concentration of <0.1 million/mL, 0% progressive motility, and <2% non-progressive motility. Morphology assessment, although difficult due to low count, suggested 0% normal forms per WHO 2021 criteria. Based on these findings, and after patient counseling, a decision was made to cryopreserve the ejaculate without extensive processing, and to thaw and use the semen sample whenever donor oocytes would become available, and then the couple would come to the clinic for an embryo transfer.
The sample contained a copious amount of debris, which ideally needed to be filtered out by Density Gradient Centrifugation (DGC), but due its poor quality, DGC was not possible. The sample was mixed with equal volumes of sperm-wash media and then centrifuged at 1500 RPM for 15 minutes. The supernatant was removed, 0.5 mL sperm wash media was added on top, and the solution was homogenized to now be frozen. Cryopreservation was performed using a slow cooling protocol with glycerol-based cryoprotectant. The goal was to retain all viable and potentially usable spermatozoa regardless of motility at the time.
On the day of donor oocyte retrieval, the sample was thawed and analyzed. Post-thaw motility was virtually absent. A direct visual scan under 400x revealed scattered twitching sperm but no progressive motility. Given the impossibility of using DGC or swim-up, we applied a technique previously described by the author [5], inspired by microfluidic sperm selection. After the semen sample was thawed, an equal volume of sperm wash media was added, the sample was homogenized and then centrifuged 1500 RPM for 15 minutes. The supernatant was discarded, and 0.5 mL of sperm-wash was added to the pellet and was homogenized again. The sample was incubated at 37°C for 30 minutes. A wide streak of 7% Polyvinylpyrrolidone (PVP) was placed on an ICSI dish and overlaid with embryo culture oil. Using a micropipette, 10 µL of the thawed semen pellet (drawn from the middle of the test tube pellet to avoid both debrisheavy bottom layers) was deposited at the base of the PVP streak. The dish was incubated at 37°C for 30 minutes.
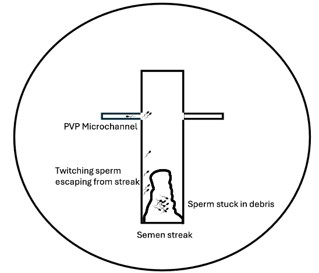
Following the initial incubation, 2 horizontal channels were drawn through the PVP streak using a finely calibrated ICSI needle (Figure 1). The dish was then returned to the incubator for a further 30 minutes. The goal of this double incubation was to reduce the viscosity of the PVP gradually, allowing twitching sperm to escape the debris-laden semen and navigate into the channels.
Under high magnification (600x), the corners of each channel were scanned. Sperm that had migrated into the channels were generally free from surrounding debris and could be visually assessed for morphology. While they were not actively motile, the fact that they separated from the debris and were now in the PVP channels confirmed their viability. Only those with an intact head, midpiece, and tail structure were selected. In cases where no sperm were found in the upper channels, scanning continued toward the base and sides of the streak.
Six donor oocytes were available for injection. Using a micromanipulator, each selected sperm was individually injected into an oocyte. Special care was taken to space out sperm within the ICSI pipette to prevent polyspermy or debris contamination. The injected oocytes were transferred to a fertilization media dish immediately following injection and incubated under standard culture conditions.
Of the six oocytes injected, five fertilized normally (83% fertilization rate). Embryos were cultured to day 5, where 3 reached blastocyst stage, including 1 grade A and 2 grade B blastocysts as per Gardner’s criteria. The embryos were frozen on 2 kitazato cryotops (1xA grade on a single cryotop, and 2xB grade on another cryotop). The female partner started her frozen embryo transfer cycle from day 1 of her next menstrual cycle where luteal support was provided using vaginal progesterone. She proceeded to have a single embryo transfer with no complications. Pregnancy was confirmed via rising beta-hCG levels and gestational sac visualization at 6 weeks. The pregnancy proceeded uneventfully, culminating in the live birth of a healthy male infant at full term.
This case report highlights the application of an innovative sperm selection technique to overcome the challenges posed by severe male factor infertility in a patient with extreme OAT. Under these circumstances, conventional sperm processing techniques such as density gradient centrifugation and swim-up are largely ineffective due to the sheer amount of cellular debris present in the sample [3], which further reduces the chances of finding motile sperm. This often leads to limited options for sperm retrieval and necessitates the use of techniques that can selectively isolate viable sperm even when motility is extremely low.
In severe-OAT samples, the presence of non-sperm cells is frequently observed. These non-sperm elements can include immature germ cells (such as spermatocytes and spermatids), leukocytes (particularly neutrophils and macrophages), and epithelial cells shed from the male reproductive tract [4]. The accumulation of leukocytes is of particular concern, as they can release Reactive Oxygen Species (ROS), leading to oxidative stress that damages sperm DNA, lipids, and proteins. High levels of oxidative stress are closely associated with reduced sperm function and impaired fertilization potential. Similarly, immature germ cells reflect disrupted spermatogenesis, while epithelial cells may indicate inflammation or infection in the reproductive tract [2]. Collectively, the abundance and types of non-sperm cells in semen not only serve as indicators of underlying testicular or accessory gland dysfunction but can also contribute directly to the pathophysiology of male infertility, and present as heavy debris in a semen sample especially post centrifugation.
The PVP-channel sperm selection technique that we employed here was inspired by the principles of microfluidics, a field in which cells are manipulated to behave according to fluid flow dynamics within microchannels. Our technique mimics this process by using a viscous PVP medium to create narrow channels that allow motile sperm to escape from surrounding debris and accumulate in the channels. This method serves as a manual alternative to costly microfluidic sperm sorting chambers, which are not always available in low-resource IVF settings. The application of this technique allowed us to visualize viable sperm in a sample that would otherwise have been deemed unsuitable for fertilization.
By reducing the viscosity of the PVP medium gradually and allowing sperm to migrate toward the channel areas, we created an optimal environment for sperm sorting based on both motility and morphology. This selective process, done under high magnification (600x), enabled the identification of viable sperm even in the presence of overwhelming cellular debris. In cases where no sperm were found in the upper channels, scanning continued through the base and sides of the streak. This allowed us to ensure that no viable sperm were missed, thereby maximizing the chances of successful sperm selection.
The successful fertilization of five oocytes and the subsequent development of three high-quality blastocysts is a testament to the effectiveness of this technique. Furthermore, the outcome of a healthy live birth demonstrates the utility of this method in overcoming male factor infertility. While the patient’s sperm quality was extremely poor, the use of the PVP-channel technique resulted in a successful ICSI cycle, which would not have been possible using traditional sperm sorting techniques.
This case report highlights the importance of embryologists in finding creative, resourceful solutions when faced with severe infertility challenges. The PVP-channel technique represents a significant advancement in the ability to select viable sperm from severely compromised samples, offering a low-cost, low-tech alternative to more expensive sperm sorting methods. While the 2021 study from Sawant used fresh OAT semen samples, this case reports using the technique for a frozen-thawed OAT sample and validates its effectiveness with the successful outcome. It also highlights the importance of adapting existing laboratory techniques to the unique needs of each patient, particularly when financial constraints or other factors limit the availability of more advanced technologies.
While this method has proven effective in the current case, further studies are needed to evaluate its reproducibility across larger cohorts of patients. Future research should focus on validating the technique’s efficacy in other clinical settings, as well as investigating its potential for improving DNA integrity and sperm quality assessments. Long-term studies examining outcomes from multiple cycles would also provide valuable insights into the long-term benefits of this approach for improving success rates in IVF.
This report underscores the clinical and scientific value of a lab-adapted PVP-channel technique in managing severe OAT cases. In the absence of motile sperm, high-magnification visual sorting combined with microfluidics-inspired sperm migration paths can enable successful fertilization and embryo development. The live birth outcome in this case confirms that even in severely compromised semen samples, innovative embryology practices can bridge the gap between biological limitation and clinical success.
Funding and conflict of interest: Authors have no funding sources and no conflicts of interest to declare.
Patient consent: Written informed consent was obtained from the patients for the use of their medical information in this case report, ensuring anonymity and confidentiality.