-
Email info@ijcmcs.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
Department of Anesthesiology and Reanimation, Division of Pain Medicine, Ankara University School of Medicine, Ankara, Hacettepe, 06230, Altindag/Ankara, Turkey
*Corresponding author: Ahmet Basari
Department of Anesthesiology and Reanimation, Division
of Pain Medicine, Ankara University School of Medicine, Ankara, Hacettepe, 06230, Altindag/Ankara, Turkey.
Email ID: dr.ahmetbasari07@hotmail.com
Tel: 05524923510
Received: Jun 18, 2025
Accepted: Jul 08, 2025
Published Online: Jul 15, 2025
Journal: International Journal of Clinical & Medical Case Studies
Copyright: © Basari A (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License
Citation: Basari A, Ozgencil GE. Radiation recall myositis resistant to conventional therapies: Clinical improvement with botulinum toxin A intervention. Int J Clin Med Case Stud. 2025; 2(2): 1024.
Background: Radiation Recall Myositis (RRM) is a rare phenomenon that occurs after radiotherapy and chemotherapy. Gemcitabine is the most commonly implicated agent in its development. Its classical treatment consists of discontinuation of the associated drug, corticosteroids, and analgesic drugs. However, there may be cases resistant to classical treatments.
Case presentation: A 49-year-old female patient treated for recurrent breast cancer developed severe pain, swelling, and muscle contracture in the left supraclavicular region after radiotherapy and gemcitabine. Despite 5 weeks of oral corticosteroid and analgesic treatment, pain and functional limitation continued. Ultrasonography and magnetic resonance imaging revealed findings compatible with myositis in the sternocleidomastoid, trapezius, and scalene muscles. Partial pain control was achieved with intralesional steroid and local anesthetic treatment. For more effective and long-term recovery, 100 IU abobotulinum toxin A was applied to the same muscle groups. Within one month, the VAS score decreased from 9 to 2, the McGill Pain Score from 92 to 20, and the need for analgesics decreased significantly.
Conclusion: RRM may sometimes not respond to classical treatments. In refractory cases, intramuscular corticosteroid and local anesthetic injections combined with botulinum toxin A can provide significant pain control and functional improvement. This case demonstrates an alternative approach to the management of treatment-resistant RRM.
Keywords: Radiation recall myositis; Gemcitabine; Botulinum toxin A; Refractory Pain; Intramuscular injection.
Radiation Recall Reaction (RRR) is a rare inflammatory reaction that occurs after systemic anticancer drugs have been administered to previously irradiated areas [1]. The most common form is dermatitis, followed by myositis [2]. In radiation Recall Myositis (RRM), swelling, redness, and pain develop in the lesion area [1,3]. Gemcitabine is responsible for most of the cases, but there are also cases reported after docetaxel, capecitabine, cyclophosphamide, carboplatin, cisplatin, mitomycin C, and 5-fluorouracil [4,5]. In RRM treatment, the plan is to first discontinue the active substance or reduce the dose according to the severity of the reaction. If symptoms persist, oral NSAIDs, corticosteroids, and antioxidant therapies are preferred [6,7]. Although a response is generally obtained within 1-2 weeks, the desired treatment efficacy may not always be achieved [2]. In this article, we present a case of RRM that developed severe pain in the cervical region after gemcitabine application and did not respond to conventional treatments. Significant improvement was observed in pain scores and daily living activities after abobotulinum toxin A injection was applied to the myositis area.
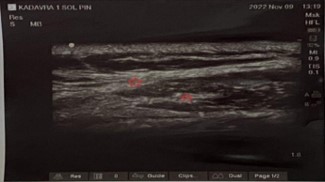
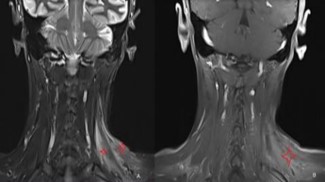
A 49-year-old female patient applied to the medical oncology unit in August 2019 due to a mass in her left breast. After the necessary tests, invasive breast cancer was detected in the biopsy, and breast-conserving surgery was performed. Afterwards, 3 cycles of docetaxel + cyclophosphamide chemotherapy and a total of 60 Gy radiotherapy in 30 fractions were given. Recurrence occurred in the same area in September 2020. After 4 cycles of doxorubicin + cyclophosphamide and 12 cycles of paclitaxel, modified radical mastectomy was performed, and oral capecitabine was started. Approximately one year later, recurrence was detected in the cervical and supraclavicular regions, and 45 Gy radiotherapy in 20 fractions and 6 cycles of gemcitabine were applied. Four weeks after the last chemotherapy, redness, pain, and swelling developed in the left supraclavicular region. In the evaluation made by medical oncology, weakness was detected in the left shoulder and upper extremity. She was referred to our pain clinic for the preliminary diagnosis of radiation-induced brachial plexopathy and pain palliation. On examination, neck deviation to the left, increased left shoulder height, and Sternocleidomastoid (SCM) muscle contracture were detected. Right neck rotation limitation, severe pain on palpation of the neck region, and color change were observed. In addition, there was moderate loss of strength in shoulder abduction and arm extension on muscle strength examination (Figure 1). McGill pain score was 92, and Visual Analog Scale (VAS) score was 9 points. In our Ultrasonography (USG) evaluation, we observed hyperechogenicity in the SCM, trapezius, and scalene muscles (Figure 2). In magnetic resonance imaging, we observed hyperintensity in the T2 phase and contrast enhancement in T1 in the same muscle groups (Figure 3). Gemcitabine treatment was stopped with the diagnosis of gemcitabine-associated radiation recall myositis. We started the treatment with drugs such as prednisolone, ibuprofen, and paracetamol + tramadol. However, despite 5 weeks of treatment, the symptoms did not regress. A 70% loss in sleep quality and daily life activities was observed due to pain. We applied dexamethasone and lidocaine to the SCM, trapezius, and scalene muscles under USG guidance. VAS decreased from 9 to 7 within a week. Afterwards, 100 IU abobotulinum toxin A was applied to the same muscles [8]. After one month, the VAS score decreased to 2. The need for analgesics decreased to 2 tablets of ibuprofen in the last month. The contracture almost completely resolved (Figure 4). The McGill score was measured as 20. Written informed consent was obtained from the patient for publication of this case report and accompanying images.


RRR is a rare phenomenon. It was first described in 1959 as a dermatitis-like inflammatory reaction that developed after actinomycin-D in a patient who underwent radiotherapy for Ewing sarcoma [9]. The reaction that occurred in many tissues and organs after radiotherapy and chemotherapy was later named RRR [10]. RRM is the most common reaction after dermatitis, which is frequently associated with gemcitabine use. The pathogenesis of RRR is not clear. However, it is thought that factors such as hypersensitivity to triggering agents in cells that survive radiation, oxidative stress, vascular structural disorders, DNA repair defects, and genetic predisposition may be effective in the development of this condition [1,10]. It is clinically characterized by muscle swelling, pain, and movement restriction. Imaging methods and laboratory tests are helpful in the diagnostic process [3,7]. Diagnosis can be made using the Naranjo Adverse Drug Reaction Probability Scale [11]. According to this scale, ≥9 points are considered definite, 5–8 points are probable, 1–4 points are possible, and ≤0 points are considered suspicious. In our patient, symptoms occurred after gemcitabine, which is the agent most commonly held responsible for the development of RRM. He received 5 points according to the probability scale, and his diagnosis was evaluated in the “possible RRM” category. In line with the treatment protocols recommended in the literature, the active agent was discontinued, and corticosteroids and NSAIDs were started. Despite medical treatment that exceeded the possible recovery period, his symptoms did not regress. Therefore, we followed a different path than the treatment modalities recommended in the literature. We applied local anesthetic and corticosteroid injections to the muscle tissues where myositis was located. When partial pain relief was achieved, we applied botulinum toxin to both reduce the contracture and provide more effective pain control. In this way, we achieved both better pain control and better functional gain. The effectiveness of the treatment approach we applied may be related to several reasons. First of all, intramuscular steroid application suppresses tissue inflammation and stabilizes nerve membranes, thus reducing pain transmission in C-fibers [12]. Local anesthetics increase tissue blood flow, thus contributing to phagocytic cells clearing damaged muscle fibers and the regeneration of muscle tissue [13]. When used together, both agents disrupt the pain cycle and reduce muscle spasm [14]. Finally, botulinum toxin-A relaxes painful muscles and breaks the pain-spasm cycle. Thus, long-term pain control is provided [15].
RRM is a rare entity. Sometimes, classical treatment approaches may not be effective. In cases that do not respond to classical treatment, intralesional steroid, local anesthetic, and botulinum toxin applications may be a more effective treatment option.
Conflict of interests: The authors declare no conflict of interest.