-
Email info@ijcmcs.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1Boston University Chobanian & Avedisian School of Medicine, USA.
2VA Boston Healthcare System, Boston, MA, USA.
*Corresponding author: H Christian Weber
VA Boston Healthcare System, Medicine Service, Section of Gastroenterology & Hepatology, Room 6A-46, 150 South Huntington Ave, Jamaica Plain, MA 02130, USA.
Email ID: christian.weber@va.gov
Tel: 857-364-4327; Fax: 857-364-4179;
Received: Jun 25, 2025
Accepted: Jul 14, 2025
Published Online: Jul 21, 2025
Journal: International Journal of Clinical & Medical Case Studies
Copyright: © Weber HC (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License.
Citation: Woodsum M, Huang K, Jati A, Weber HC. Hemothorax from bleeding paraesophageal varices: A rare complication of cirrhosis. Int J Clin Med Case Stud. 2025; 2(2): 1025.
Spontaneous hemothorax from paraesophageal variceal hemorrhage is a very rare complication of cirrhosis. Our report highlights a patient with previously compensated cirrhosis hospitalized with acute alcoholic hepatitis and newly decompensated cirrhosis. The patient developed acute hypoxic respiratory failure with new significant anemia. CT imaging demonstrated a mediastinal hematoma and large hyperdense pleural effusion consistent with hemothorax from paraesophageal variceal bleed. No intraluminal GI bleeding was noted and hemothorax was confirmed with thoracentesis. TIPS and chest tube drainage were proposed but her condition declined, and she passed away after transitioning to comfort measures.
A 62-year-old female with a history of Alcohol Use Disorder (AUD), compensated cirrhosis secondary to alcohol use, and major depressive disorder presented to the hospital with several days of large volume watery diarrhea, abdominal pain, jaundice, and pleuritic chest pain. She denied fevers, chills, dizziness, dyspnea, hematuria or dysuria and reported no hematemesis, melena, or hematochezia. She had been drinking 1 pint of vodka daily for 2 years following 10 years of sobriety when symptoms began but denied any signs of alcohol withdrawal. She was not taking any medications.
On clinical examination, vital signs were notable for tachycardia but were otherwise normal. She was alert and oriented but ill-appearing with jaundice and scleral icterus. Breath sounds were clear to auscultation bilaterally. Her abdomen was tender in the right upper quadrant, had no appreciable ascites, and she had no asterixis.
Initial labs included white blood cell count 9,300 /uL, hemoglobin of 10.9 g/dL, platelet count 135,000 /uL, sodium 135 mmol/L, creatinine 0.93 mg/dL, albumin 1.8 g/dL, aspartate aminotransferase 210 U/L, alanine aminotransferase 36 U/L, alkaline phosphatase 388 U/L, total bilirubin 22.1 mg/dL, prothrombin time 22.3 seconds, and INR 1.9. Her calculated MELD-Na score was 27, and Maddrey’s Discriminant Function was 69.5. A stool sample tested positive for Clostridium difficile toxin B by PCR.
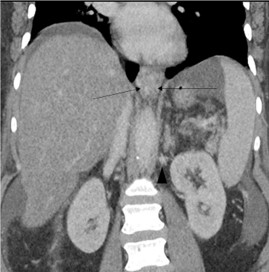
CT angiogram of the chest was negative for a pulmonary embolism or pneumonia. Abdominal CT demonstrated a cirrhotic appearing liver with mild ascites, paraesophageal varices, and recanalization of the umbilical vein consistent with collateral venous flow in the setting of portal hypertension (Figure 1).
The patient was started on PO vancomycin for Clostridium difficile colitis. Steroids for alcoholic hepatitis were deferred in the setting of infection. Ascites from a diagnostic paracentesis was not consistent with spontaneous bacterial peritonitis. Despite maximal supportive care, her liver transaminases, bilirubin, and INR continued to rise.
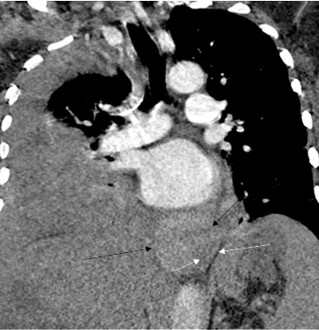
On hospital day ten, she developed acute dyspnea and hypoxia requiring supplemental O2. The hemoglobin was 6.2 g/ dL, declined from 8.6 g/dL 24 hours earlier. The patient had no hematemesis, melena, or hematochezia. CT pulmonary angiogram demonstrated a large right pleural effusion (Figure 2) and a new 9.5 × 3.6 × 5.0 cm large heterogeneous hyperdense lesion in the lower posterior mediastinum abutting the esophagus consistent with a mediastinal hematoma. No pneumomediastinum was seen to indicate an esophageal rupture. Diagnostic thoracentesis confirmed hemothorax with return of frank blood. The patient was subsequently intubated and transferred to the intensive care unit, where she was placed on vasopressors and initiated on massive transfusion protocol for hemorrhagic shock. No bloody output was noted from her orogastric tube or her rectum. Repeat CT angiogram six hours later revealed interval enlargement in the mediastinal hematoma to 10 × 7.4 × 3.8 cm and dependent higher density fluid suggesting blood in the right pleural effusion. Extensive posterior mediastinal paraesophageal varices were demonstrated but no active extravasation was noted.
These findings were consistent with venous bleeding from paraesophageal varices leading to hemothorax causing hemorrhagic shock and respiratory failure. A multidisciplinary discussion with interventional radiology, gastroenterology, critical care, and thoracic surgery concluded with a plan for Transjugular Intrahepatic Portosystemic Shunt (TIPS) to address the portal hypertensive bleeding, as well as chest tube placement to drain her hemothorax. However, her condition rapidly declined further and she passed away shortly after transitioning to comfort measures in accordance with the family’s wishes.
This case highlights an exceptionally rare variation of extraluminal portal hypertensive bleeding from paraesophageal varices only documented in three previous reports [1-3]. Esophageal varices are formed when portal hypertension reverses blood flow from the portal venous system into the left gastric vein that feeds the esophageal venous plexus [4]. Increased pressure can lead to development of varices not only in submucosal esophageal veins but also extraluminal paraesophageal veins.
Paraesophageal Varices (PEVs) arise from veins that course parallel to, but exist distinct from, the esophageal wall. PEVs are seen on CT in 22-38% of patients with portal hypertension and portend a poor prognosis [5-7]. Endoscopic ultrasound studies illustrated PEVs feeding into esophageal varices via perforating veins, and some suggest they may play a role in recurrence of esophageal varices [8]. However, PEVs themselves are rarely implicated as the source of bleeding.
The other case reports describing hemothorax from bleeding PEVs all occurred in patients with decompensated alcoholic cirrhosis, and shared CT findings of a hyperdense mediastinal hematoma with adjacent hemothorax [1-3]. One case closely mirrored ours as it occurred in the setting of alcoholic hepatitis [3]. Acute worsening of portal hypertension is directly mediated by alcoholic hepatitis by increasing portal inflow, increasing intrahepatic vasoconstriction, inflammation, and changing liver vasculature [9,10]. These changes likely precipitated the development and rupture of PEVs in these cases. Portal hypertension was further exacerbated in our case due to inability to treat alcoholic hepatitis due to her concurrent infection, and lack of beta blockade.
However, portal hypertension alone does not explain why these patients presented with hemothorax instead of the usual intraluminal esophageal variceal bleeding. No hematemesis or melena was noted in any of the cases, and the two cases in which endoscopy was performed revealed either no varices or grade 1 varices [1,3]. Varices tend to develop in the distal esophagus because the veins in this area (known as the palisade zone) lack perforating veins that drain into periesophageal and azygous veins [4]. Variations in normal vascular anatomy could explain the propensity for PEVs in certain patients.
No official recommendations exist to guide management when these varices are discovered. More aggressive measures to lower portal pressures upon discovery of PEVs, such as earlier initiation of beta blocker or TIPS, could have changed the clinical outcome of our patient and may be considered in future guidelines. Although our patient was too ill to undergo such measures, TIPS and/or thoracotomy with direct ligation of bleeding vessels have been successfully used to address intrathoracic portal hypertensive bleeding [2,11-14]. The described imaging findings in the presence of rapid decline in hemoglobin and lack of intraluminal GI bleeding signs should prompt the suspicion for this rare cause of bleeding.
Conflicts of interest: All authors have no conflicts of interest.