-
Email info@ijcmcs.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
1ECS.Education, Sweden.
2Tshwane University of Technology, University of Pretoria, ECS.Education, Cannabis Research Council, Society of Cannabis Clinicians, Holistic Integrative Healing Institute, South Africa.
*Corresponding author: Shiksha Gallow
Tshwane University of Technology, University of
Pretoria, ECS.Education, Cannabis Research Council, Society of Cannabis Clinicians, Holistic Integrative Healing Institute, South Africa.
Email ID: drgallow@hihealing.co.za
Received: Jul 09, 2025
Accepted: Aug 04, 2025
Published Online: Aug 11, 2025
Journal: International Journal of Clinical & Medical Case Studies
Copyright: © Gallow S (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License
Citation: Broselid S, Gallow S. Bridging the gap: Integrating the endocannabinoid system into medical education. Int J Clin Med Case Stud. 2025; 2(2): 1027.
This study addresses the critical gap in medical education concerning the Endocannabinoid System (ECS), a key component of physiological regulation absent from standard medical curricula. Despite its discovery in 1992 and its established role in maintaining homeostasis, the ECS is largely ignored in medical training, affecting patient care, therapeutic development, and clinicians’ grasp of physiology. Recent shifts in cannabis legislation and emerging ECS-targeted therapies underscore the urgency of integrating ECS education into healthcare training. A bibliometric analysis comparing ECS related publications to other physiological systems reveals that the ECS significantly influences biomedical research, with a high h-index and citation frequency. These findings highlight the need for curricular reforms that address this underrepresented but vital system, equipping future healthcare providers with a comprehensive understanding of human physiology.
Executive summary
This article highlights a significant oversight in modern medical education: the absence of the Endocannabinoid System (ECS) from standard medical curricula and textbooks. Despite its discovery in 1992 and its crucial role in maintaining physiological homeostasis, the ECS remains largely unaddressed in medical training. This omission, particularly in light of recent cannabis legislation changes and emerging therapeutic applications, has profound implications for patient care, drug development, and our healthcare providers’ comprehensive and accurate understanding of human physiology.
The endocannabinoid system: A brief overview
The ECS is a complex cell-signaling system involved in regulating a wide range of physiological processes, including
• Pain perception [1]
• Mood regulation [2]
• Appetite and metabolism [3]
• Immune function [4]
• Sleep [5]
• Memory and learning [6]
Its importance in maintaining bodily homeostasis cannot be overstated, as it interacts with nearly every major physiological system [7].
The problem: A glaring omission
A title-based biblometric analysis was conducted using Pubmed and Google Scholar.
A comparative analysis of physiological systems, as depicted in table 1, revealed the following:
• 1,201 publications in PubMed contain ‘Endocannabinoid System’ in their titles.
• 1000 such publications garner 76,843 total citations (Google Scholar).
• 1000 such publications boast an h-index of 138, surpassing several well-established physiological systems including the digestive, endocrine, and respiratory Systems.
This data underscores the ECS’s significant impact and influence in biomedical research, highlighting the dangerous disconnect between its scientific importance and its lack of representation in medical education.
| Physiological system | Title-based publications (PubMed) | Total citations* (Google Scholar) | h-index* (Google Scholar) |
|---|---|---|---|
| Endocannabinoid system | 1,201 | 76,843 | 138 |
| Digestive system | 958 | 38,121 | 77 |
| Immune system | 7,985 | 354,807 | 309 |
| Endocrine system | 374 | 23,848 | 74 |
| Cardiovascular system | 2,088 | 103,097 | 167 |
| Respiratory system | 909 | 35,628 | 83 |
| Lymphatic system | 373 | 23,885 | 76 |
| Nervous system | 26,875 | 336,911 | 306 |
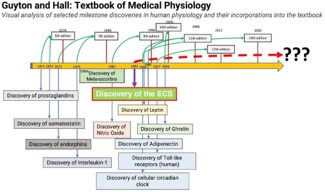
A visual analysis of the Guyton and Hall Textbook of Medical Physiology, a cornerstone of medical education, as depicted in figure 1, revealed the following key findings:
• Consistent incorporation of various physiological discoveries since the 1970s.
• The conspicuous absence of the ECS, despite its discovery in 1992.
• This omission persists even in the most recent 2020 edition.
Global knowledge gap among healthcare professionals
| Article | Country | HCP | Opinions on CBMPs | Knowledge level and gaps | Barriers for increased medical use and prescription of CBMPs |
|---|---|---|---|---|---|
| Jankie et al. (2023) |  |
Medical students | Perceived benefits for chronic pain, anxiety, seizures; low risk identification | Difficulty identifying indications and adverse effects; curriculum lacks cannabis info | Unprepared to answer patient queries (85.8%) |
| Rosenbæk et al. (2023) |  |
GPs | Majority hold negative view on MC prescription; 8.7% have experience | 80.6% have little or no knowledge about MC | Negative attitudes, few GPs willing to prescribe |
| Bawa et al., (2022) |  |
GPs | Supported MC in palliative care, cancer pain, nausea, epilepsy; less for mental health, insomnia | 66.9% felt inadequate knowledge | 1 in 5 prescribed MC; 52.3% comfortable discussing with patients |
| Parmelee and Clark, (2022) |  |
Nursing students | Positive opinions; lack of education | Few students receiving cannabis education | Nursing programs lack education |
| Jacobs et al., (2022) | |
Medical students | Mixed attitudes toward legalization; desire for MC education | Erroneous beliefs; unreliable info sources | Minimal training in MC |
| Sokratous et al., (2022) |  |
Nurses | MC acceptable for certain indications | Lack of knowledge on risks and benefits | Need for enriched nursing curricula |
| de Santiago Moraga, J. (2022) |  |
Pain Physicians | 38% find MC effective, 78% safe | 95% felt they need specific training | 47% need specific unit, 34% need specialist for prescription |
| Akiki et al., (2023) |  |
Physicians | 80% support decriminalization; 16% know indications, 24% know secondary effects | Lacked knowledge and confidence | Lack of formal education |
| Adler et al., (2022) |  |
Primary care physicians | 51% find MC effective | 63% have little knowledge; 75% want to deepen it | <50% willing to initiate MC treatment; willingness varies |
| Kruger et al., (2022) | |
HCPs | Moderate knowledge; 58% correct | Low knowledge; barrier to recommendations | Lack of knowledge and awareness |
| Orjuela-Rojas et al., (2021) |  |
Psychiatrists | Favorable attitude; lack of knowledge on legal status and access | Lack of knowledge on legal status and access | Barriers to legal access |
| Filetti et al. (2021) |  |
Oncologists, palliative care physicians | Discrepancy between attitudes, prescription, knowledge | Attitudes and prescription don't match knowledge | Need for education programs, national guidelines |
| Karanges et al. (2024) | |
Medical practitioners | Generally positive attitudes; 21.9% prescribed MC | Limited knowledge and confidence | Regulatory barriers, concerns about driving, mental health risks |
| Zylla et al. (2023) | |
Oncology clinicians | Majority support MC use for cancer symptoms | Knowledge gaps in dosing, drug interactions | Lack of high-quality evidence, concerns about side effects |
| Mirzayov et al. (2024) | |
Medical students | 79.4% agreed there was a role for medical cannabis in healthcare; 52.5% would agree to be licensed to prescribe | Not measured. | Most medical students support the use of medical cannabis for medical purposes and are in favor of its legalization. |
| Rønne et al. (2021) |  |
Hospital physicians and GPs | 10-95% willing to prescribe, depending on setting, specialty, and experience | General lack of knowledge of clinical effects (both beneficial and adverse) | Lack of knowledge of effects and how to advise patients; skepticism among addiction specialists |
| Zolotov et al. (2021) | |
Medical students | Varied attitudes; need for more education | Limited knowledge; need for more education | Lack of formal education; need for curriculum development |
| Weisman et al. (2021) | |
Medical students and professionals | Increasing acceptance of MC over time; strong desire for more education | Knowledge gaps; desire for more educational material | Restrictive policies; stigma; misinformation |
A comprehensive review of recent studies revealed a widespread lack of ECS knowledge among healthcare professionals globally, as shown in table 2:
• 80.6% of Danish General Practioners (GP) reported little to no knowledge about medical cannabis, indicating a likely gap in ECS understanding (Rosenbæk et al. 2023),
• 66.9% of Australian GPs felt their knowledge was inadequate (Bawa et al. 2022).
• 95% of Spanish pain physicians felt they needed specific training (de Santiago Moraga 2022).
• In the United States, medical students demonstrated erroneous beliefs and relied on unreliable information sources regarding medical cannabis (Jacobs et al. 2022).
This global trend highlights a systemic failure in medical education to address the ECS, despite its critical physiological importance.
Incomplete medical knowledge: Graduating medical professionals lack a comprehensive understanding of human physiology, as evidenced by the bibliometric analysis and global knowledge gap.
Missed therapeutic opportunities: The ECS’s potential as a therapeutic target remains largely unexplored in mainstream medicine, as shown by the textbook analysis and healthcare professionals’ lack of knowledge.
Suboptimal treatment options: Without training, clinicians might not be aware of medical cannabis as a treatment option for conditions like chronic pain, epilepsy, or cancer-related symptoms, resulting in reliance on potentially less effective or more harmful treatments.
1.Improper use: Patients may use medical cannabis without proper guidance, leading to potential misuse, adverse effects, or drug interactions. This can be particularly risky for those with complex medical conditions or those on other medications.
2.Lack of monitoring: Healthcare professionals may be less equipped to monitor and manage the effects and side effects of medical cannabis if they are not trained, leading to potential complications or suboptimal patient outcomes.
3.Diagnostic gaps: Conditions influenced by ECS dysfunction may be misunderstood or misdiagnosed due to the omission of ECS from medical education.
4.Inequity in patient access: Patients may face disparities in access to medical cannabis treatments due to varying levels of physician knowledge and comfort with prescribing or recommending these therapies.
5.Stunted drug development: Pharmaceutical research may overlook promising avenues for new treatments, as indicated by the discrepancy between research output and educational content.
6.Limited research: Without a focus on medical cannabis in curricula, there may be fewer opportunities for research into its efficacy, safety, and best practices. This can slow the advancement of knowledge and innovation in the field.
7.Lack of expertise: Future healthcare professionals may lack the expertise to contribute to ongoing research or to advance the scientific understanding of medical cannabis and its applications.
8.Patient care impact: Patients may not receive optimal care due to healthcare providers’ limited knowledge of the ECS, as demonstrated by the global knowledge gap.
9.Delayed medical cannabis adoption: To understand the therapeutic potential and efficacy of medical cannabis, a basic understanding of the ECS is necessary, which is currently lacking among healthcare professionals worldwide.
10.Inadequate preparation: Medical schools and training programs that do not include medical cannabis may inadequately prepare students for real-world scenarios where they encounter patients using or asking about medical cannabis.
11.Professional development: Continuing education and professional development opportunities may be limited for those seeking to expand their knowledge of the ECS and/or medical cannabis if it is not integrated into the core curriculum.
1.Stigma: The ECS’s association with cannabis may have led to unwarranted stigmatization, as suggested by the textbook analysis and healthcare professionals’ attitudes.
2.Inertia in medical education: The slow integration of new discoveries into established curricula, as evidenced by the textbook analysis and global knowledge gap.
3.Lack of awareness: Limited recognition of the ECS’s importance among medical educators and policymakers, despite its significant research impact shown in the bibliometric analysis.
Curriculum reform: Integrate ECS education into medical school curricula and continuing medical education programs to address the global knowledge gap.
1.Textbook updates: Urge medical textbook publishers to include comprehensive ECS information in future editions, as the current omission is evident in the textbook analysis.
2.Research funding: Increase support for ECS research to further elucidate its role in health and disease, building on the already significant research output.
3.Public awareness: Launch campaigns to educate the public and healthcare professionals about the ECS, addressing the widespread lack of knowledge.
4.Policy changes: Advocate for the inclusion of ECS knowledge in medical licensing exams and accreditation standards to ensure future healthcare professionals are adequately informed.
The omission of the Endocannabinoid System from medical education represents a significant gap in our approach to healthcare. This oversight is evident in the bibliometric analysis, textbook content, and the global knowledge gap among healthcare professionals. Addressing this issue is crucial for advancing medical knowledge, improving patient care, and unlocking new therapeutic possibilities. It is imperative that the medical community, educators, and policymakers take immediate action to integrate ECS education into the core of medical training and practice.