-
Email info@ijcmcs.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
Department of Pediatric Surgery, Woman, Mother and Child Hospital, CHU of Martinique, France.
*Corresponding author: Djeradi Ahyee
Department of Pediatric Surgery, Woman, Mother and
Child Hospital, CHU of Martinique, France.
Email ID: djeradi02@gmail.com
Received: Jul 10, 2025
Accepted: Aug 06, 2025
Published Online: Aug 13, 2025
Journal: International Journal of Clinical & Medical Case Studies
Copyright: © Ahyee D (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License
Citation: Ahyee D, Patrick W, Assan BR, Ebassa K, Sommier J, et al. Nodular fasciitis in a child: A case report of an unusual localisation and literature review. Int J Clin Med Case Stud. 2025; 2(2): 1028.
We report a rare case of nodular fasciitis in a 12 years old boy. He noticed a rapidly growing swelling in the left supraclavicular region over 6 months. MIR of the shoulder showed a well-limited oval tissue mass within the insertion of the trapezius muscle on the clavicle, taking contrast after gadolinium injection with no signal abnormalities in muscle and bone tissue.
Biopsy was performed and showed medium-sized spindle cells with myofibroblastic differentiation expressing smooth muscle actin in favor of nodular fasciitis. FISH (Fluorescent in Situ Hybridization) showed a rearrangement involving USP6 gene confirming the diagnosis. Nodular Fasciitis (NF) is a rare and benign soft-tissue mass often misdiagnosed as a malignant neoplasm because of it fast and infltrative growth pattern. It should be thought in front of soft-tissue mass with fibroproliferative lesions to avoid misdiagnosis and overtreatment.
Nodular Fasciitis (NF) is a rare and benign soft-tissue mass often misdiagnosed as a malignant neoplasm because of it fast and infltrative growth pattern. It is considered as a reactive process that involves the proliferation of mesenchymal origin cells, such as fibroblasts and myofbroblasts [1]. In adults, NF occurs most commonly in the upper extremities. It can be found at any age and common in adults aged 20-40 years [2]. Its prevalence in children is low, accounting for only 10% of reported cases [3]. In the pediatric population, although NF is most commonly reported to occur in the head and neck, its location may vary. NF was first described as pseudosarcomatous fasciitis by Konwaller et al. in 1955, however, the pathogenesis of NF remains unknown [3]. It often affects histological features [1], similar to subcutaneous and rarely periosteal [3].
Particular localisation had been reported in the orofacial region, in the skin of the face, parotid gland, buccal mucosa, labial mucosa, and tongue [6,7].
We present an unusual presentation of supraclavicular nodular faciitis in a child of 12 years old.
A 12 years old boy was admited with a non febril and painless swelling of the left supraclavicular region. He noticed a rapidly growing swelling in the left supraclavicular region over 6 months. It started with pain at the begining in the supraclavicular region with stretch mark lesions. There is no prior known history of traumat or infection or wound of the region. We noticed that there was a second cousin in the family treated for an hypothalamic-chiasmatic pilocytic astrocytoma.
Physical examination revealed a child in an excellent general condition with a left supraclavicular mass non swelling and painless with stretch mark lesions. It was a mobile, firm mass, fixed to the deep plane and in relation to the skin (Figures 1). There was no active and passive shoulder limitation, no lymphadenopathy. We noticed some spots on the buttock and the back of the shoulder. Biological tests including hemogram were normal.
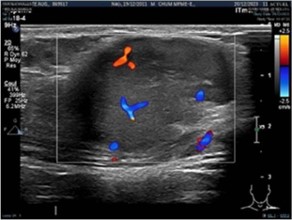
Ultrason showed a well-limited tissue mass of (39 × 23 × 21 mm) within the vascularized trapezius muscle on doppler (Figures 2).
Magnetic Resonance Imaging (MIR) of the shoulder showed a well-limited oval tissue mass of 45 mm diameter within the insertion of the trapezius muscle on the clavicle, taking contrast after gadolinium injection with no signal abnormalities in muscle and bone tissue (Figure 3).
Cerebral and abdominopelvic scan were normal. After discussion about the clinical picture, a biopsy was performed and showed medium-sized spindle cells with myofibroblastic differentiation expressing smooth muscle actin in favor of nodular fasciitis. FISH (Fluorescent in Situ Hybridization) showed a rearrangemnt involving USP6 gene confirming the diagnosis.



| Authors and country | Age and gender | Time before diagnosis | Localisation | Dignosis | Surgery | Outcome |
|---|---|---|---|---|---|---|
| Lääveri et al., Finlande, 2017 | 7 ans (F) | 1 mois | Left hemimandible | Ultrasson/CT-SCAN/MIR/Anatomopath | Yes | Good |
| Eida et al., Japon, 2021 | 11 ans (F) | 2 semaines | Left hemimandible | X-ray/CT Scan/MIR/Anatomopathology | Yes | Good |
| Antunes et al., Portugal, 2013 | 17 mois (F) | 1 jour | Cervical region | CT Scan/Anatomopathology | No | Good |
| Chen et al., Chine 2020 | 3 ans (F) | left nasal cavity | CT Scan/MIR/Anatomopathology | Yes | ||
| Lenyoun et al., Etats Unis, 2008 | 3 mois (F) | 1 mois | Left cheek | CT Scan/Anatomopathology | Yes | Good |
| Halsey et al., Etats Unis, 2020 | 9 mois (M) | Ear | No | Good | ||
| Taleuan et al., Maroc, 2018 | 16 ans (F) | 2 ans | Left mandible angle | X-ray/CT Scan/MIR/Anatomopathology | Yes | Good |
| Haddad et al, Canada, 2001 | 9 ans (F) | 3 semaines | Upper commissural region (upper lip) | Anatomopathology | Yes | Good |
| Volpe et al., Italie, 2022 | 4 ans (F) | Left ear | CT Scan/MIR/Anatomopathology | Yes | Good | |
| Suh et al., Corée, 2014 | 16 ans (G) | 2 mois | Left anterior hemithorax | CT Scan/AAnatomopathology | Yes | Good |
| Seo et al., Corée, 2014 | 18 ans (F) | Chance discovery | Right fifth intercostal space | CT Scan/Anatomopathology | Yes | Good |
| Ko et al., Taïwan, 2013 | 4 ans (F) | 4 mois | Intra-articular right knee | MIR/Anatomopathology | Yes | Good |
| Liu et al., Chine, 2021, | 17 mois (F) | 4 mois | Concha of the right ear | Anatomopathology | Yes | Good |
| Dworak et al., Etats unis, 2021 | 16 ans (M) | 4 mois | left periorbital | CT Scan/AAnatomopathology | Yes | Good |
| Chan et al., Singapour, 2014 | 17 ans (M) | 2 mois | Right knee | MIR/Anatomopathology | Yes | Good |
| Patel at al., Etats unis, 2021 | 12 ans (F) | 6 mois | Near the right eye (zygomatic region) | Anatomopathology | Yes | Good |
| Mazura et al., Etats unis, 2012 | 11 ans (F) | 2 mois | Right major | Ultrason/CT Scan/MIR/Anatomopathol | Yes | Good |
| Hara et al., Japon, 2010 | 17 ans (M) | 1 mois | First interdigital space of the right hand | X-ray/CT Scan/MIR/Anatomopathology | Yes | Good |
| Wang et al., Chine, 2021 | 3 ans (F) | 1,5 ans | Right ear | Ultrason/CT Scan/MIR/Anatomopathol | Yes | Good |
| Wang et al., Chine, 2021 | 17 mois (M) | 4 mois | Right ear pinna | Ultrason/MIR/Anatomopathology | Yes | Good |
| Wang et al., Chine, 2021 | 19 mois (M) | 6 mois | Left ear pinna | Ultrason/CT Scan/MIR/Anatomopathol | Yes | Good |
Nodular Fasciitis is defined by the WHO as a benign and probably reactive nodular fibroblastic growth. It can be found at any age and common in adults aged between 20-40 years [2]. Its prevalence in children is low, accounting for only 10% of reported cases [2]. The lesion appeared as a homogeneous tissu mass. All clinical presentation in the literature are reported cases (Table 1).
Location
Though common locations described are the upper extremities (48%), the trunk (20%) and less frequently (10-20%) the head and neck [4], the literature refers to certain particular locations as ear cavity, periorbital region, mandible, nasal cavity, intre-articular cavity [2,3,6,8,9]. Our clinical case report a supraclavicular presentation of nodular faciitis in a child. This location had not been yet reported in literature.
Etiology
Initially considered secondary to a trauma, this theory was discarded because there were no history of trauma with all the patient with nodular fasciitis [4].
Clinical presentation
Nodular Fasciitis’s clinical presentation is rather unspecific; the most common presentation is a solitary, rapidly growing solid mass, with frequently or not associated pain and tenderness. Lesions can vary in size, from 0.5 cm to 10 cm, but most are lower than 2-4 cm [4]. With our clinical presentation, the location of the mass, the pain and the duration of evolution made us think of a probably malignant tumor or a Virchow node.
Imaging features
Imaging features can help characterise the lesion and the surrounding anatomy but are also unspecific and, most of the times, insufficient to make the correct diagnosis or differentiate it from malignant lesions. MRI of Nodular Fasciitis shows various signal intensities, probably because of the combination of variability in cellularity. In general, the signal intensity of the lesion with myxoid or cellular histology is higher than that of muscle on T2-weighted images, whereas lesions with fibrous histology present as a markedly hypointense signal compared with the surrounding muscles on all pulse sequences. The coexistence of abundant collagen and a cellularity in the fibrous lesions leads to a reduction in signal intensity on T2-weighted images [2].
MIR features in our case contrast-enhanced using gadolinium revealed increased heterogeneous enhancement which are similar to MIR description in nodular fasciitis reported in the literature [2,4,10].
Histological examination
Nodular Fasciitis arising from subcutis and within muscle often extend between fat cells and muscle cells, respectively. It can be presented as myxoid, granuloma or fibroma tissu and can change during the progressing of the disease. On the microscopic level nodular fasciitis is characterized by the presence of fleshy, regular spindle cells with a type of cellular culture [8].
We observe in this lesion a type of tumoral cell proliferation with immature fibroblastic lesions and rich mitotic activity that may be confused with sarcoma [4]. Most authors agree on the certainty of nodular fasciitis diagnosis, in the presence of USP6 gene rearrangement with a sensibility and a specificity of respectly 93% and 100% [4-8-9]. In our case the lesion was developed at the expense of the left trapezius muscle and histological examination was in line with literature data.
Treatment
The literature mentions surgical resection as being the appropriate treatment with a good prognosis. Recurrences are rare and mainly due to incomplete excisions [2,3]. In addition to surgical resection Chen and All proposed intratumor injection of triamcinolone [6].
If asymptomatic lesions may be treated non operatively, in our case clinical findings and no complains of the patient and the lak of surgical criteria evidence to put our patient under a surgery made us choose for non-surgical management. After 06 months our patient has been seen. Physical examination revealed a child in a excellent general condition with wellpreserved range of motion and no pain. We noticed a considerable reduction in mass (Figure 4).
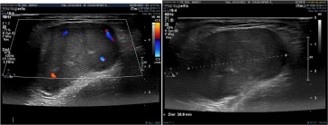
Ultrason showed a serious decrease of (30 × 22 × 22 mm) in mass size (Figure 5). The patient continue going to school and perform all physical activities.
We will continue our following do detect and consider any abnomalities.
Nodular Fasciitis (NF) is a rare and benign soft-tissue mass often misdiagnosed as a malignant neoplasm because of it fast and infltrative growth pattern.
Its prevalence in children is low, accounting for only 10% of reported cases.
No significant regression without surgery has been reported in the literature. In the pediatric population, a variable presentation has been reported in the literature and all went under surgery. Nodular fasciitis should be thought in front of soft-tissue mass with fibroproliferative lesions to avoid misdiagnosis and overtreatment.