-
Email info@ijcmcs.org
-
Address 848 N. Rainbow Blvd. #5486 Las Vegas, NV 89107, USA
Urology Department, Guys and St Thomas NHS Trust, UK.
*Corresponding author: Youssef Ibrahim
Urology Department, Guys and St Thomas NHS Trust, UK.
Email ID: youssef.ibrahim2@nhs.net
Received: Aug 02, 2025
Accepted: Aug 25, 2025
Published Online: Sep 01, 2025
Journal: International Journal of Clinical & Medical Case Studies
Copyright: © Ibrahim Y (2025). This Article is distributed under the terms of Creative Commons Attribution 4.0 International License.
Citation: Ibrahim Y, Gad M, Mokbel S, Nair R, Thurairaja R, et al. Robotic enucleation for large inflammatory myoblastic tumour: A safe, margin-conscious approach to maximise bladder preservation. Int J Clin Med Case Stud. 2025; 2(2): 1031.
Inflammatory Myofibroblastic Tumour (IMT) of the bladder is a rare mesenchymal neoplasm with low malignant potential. While typically managed with organ-sparing surgery, large or exophytic lesions pose a challenge due to the risk of bleeding, local progression, and potential infiltration of adjacent structures. We report the case of a 59-year-old male presenting with acute clot retention secondary to an 8 cm bladder mass. Initial transurethral biopsy resulted in severe haemorrhage and iatrogenic bladder perforation, necessitating intensive care admission. Histology was inconclusive, but immunohistochemistry later confirmed IMT with ALK gene rearrangement. The patient underwent robotassisted enucleation of the bladder mass. Intraoperatively, the lesion appeared well-encapsulated with a clear dissection plane, allowing complete excision while preserving bladder capacity and avoiding ureteric reimplantation. Recovery was uneventful. Final histopathology confirmed IMT. At 3-month follow-up, the patient remained recurrencefree on MRI and cystoscopy, with preserved bladder capacity and minimal urinary symptoms.
Inflammatory Myofibroblastic Tumour (IMT) of the bladder is a rare mesenchymal neoplasm with low malignant potential. Patients often present with painless haematuria or storage lower urinary tract symptoms, although some experience only vague symptoms [1,2].
Histologically, IMT consists of spindle myofibroblastic cells with a polymorphous inflammatory infiltrate. Immunohistochemical staining is essential in confirming the diagnosis with 50-65% harbouring rearrangements of the ALK gene [3].
Despite favourable prognosis, complete surgical excision is the recommended treatment in all cases due to risk of bleeding, local progression and infiltration into the surrounding structures. Distant metastasis is exceedingly rare [4]. Most bladder IMTs can be managed with organ-sparing surgery— typically transurethral resection or partial cystectomy—thus avoiding more radical interventions [5]. Minimally invasive approaches such as laparoscopic or robot-assisted partial cystectomy for IMT have been reported with good outcomes [6].
We present a case of a relatively large IMT of the bladder managed by robotic enucleation with good short term oncological and functional outcome at 3 months.
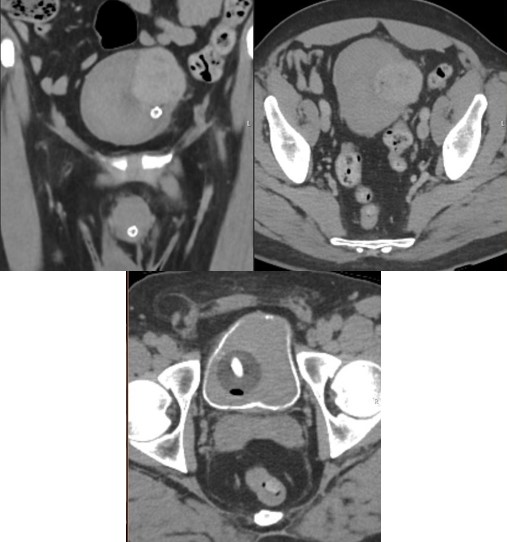
A fifty-nine-year-old male with no significant past medical history was admitted through accident and emergency to the referring hospital with acute clot retention. Initial conservative management with manual bladder washouts and continuous bladder irrigation, via three-way catheter, was unsuccessful, with ongoing transfusion dependent haematuria. An urgent CT urogram showed a solid 8 cm bladder mass and extensive intravesical clots (Figure 1).
Local urology team proceeded to perform rigid cystoscopy and bladder washout under general anaesthesia. Intra-operative attempt of resection biopsy resulted in severe bleeding necessitating intra-operative transfusion of four units of packed RBCs. Bleeding was difficult to control endoscopically and was complicated by iatrogenic bladder perforation.
Ureteric stents were inserted in both ureters and externalized for urinary diversion alongside a 3-way urethral catheter with continuous bladder irrigation and patient was transferred to the intensive care unit for close monitoring, stabilization and repeat cross-sectional imaging.
Repeat CT urogram confirmed large solid bladder mass with no significant extravesical fluid collection. Patient remained haemodynamically stable without further transfusion. Conservative management was continued while awaiting histopathology. Initial histology was inconclusive, consisting of multiple spindle cell fragments, raising suspicion for a sarcomatoid lesion and prompting urgent immunohistochemical analysis which later suggested IMT with ALK gene rearrangement.
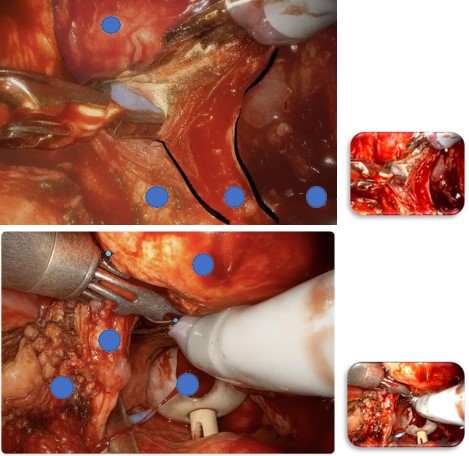
The patient subsequently had cystoscopy, left JJ stent insertion, and robot-assisted enucleation of the bladder mass. Intraoperatively, the lesion appeared well encapsulated with well demarcated margin between the bladder muscle and the mass. Therefore, mass was enucleated to maximise bladder preservation and avoid need for ureteric reimplantation. This entailed combination of sharp and blunt dissection to peel the lesion off the bladder wall (Figure 2).
A drain was placed at the end of the procedure which was removed next day. Patient was discharged on day 2 after the procedure with catheter in-situ. Cystogram performed 3 weeks later showed no leak and had successful the trial without catheter.

On final assessment tumour was composed of pleomorphic spindle and epithelioid cells with large nuclei, prominent nucleoli, and occasional intracytoplasmic inclusions. The tumour architecture was heterogeneous, showing interlacing fascicles and alveolar-like patterns. Mitotic activity was present (up to 4 per 10 high-power fields), but without atypical features. Immunohistochemistry showed tumour cell positivity for MNF116, AE1/AE3 (cytoplasmic), ALK-1, SMA (patchy), desmin, p53 (wildtype expression), caldesmon, focal calponin, and vimentin, with a high Ki-67 proliferation index. The tumour was negative for 34βE12, EMA, S100, CD31, CD34, D2-40, myogenin, and calponin. These findings were consistent with an Inflammatory Myofibroblastic Tumour (IMT) exhibiting florid/reactive features.
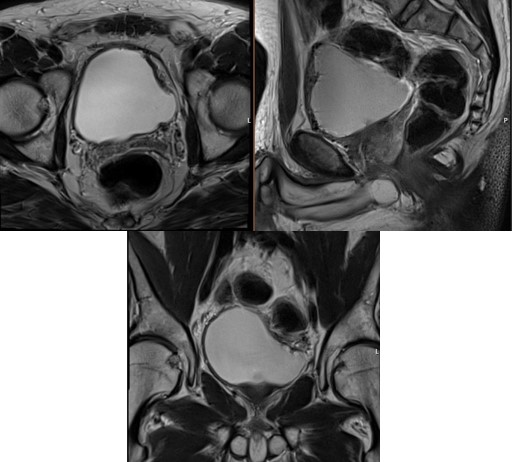
Follow-up at 3 months with MRI and flexible cystoscopy confirmed no evidence of recurrence (Figure 4). The patient maintained a satisfactory functional bladder capacity (300 ml) and reported an International Prostate Symptom Score (IPSS) of 5 with a storage score of 0.
IMT is a benign lesion with a generally favourable prognosis. Complete surgical excision typically results in excellent local control and long-term survival. This study presents a novel surgical approach for the management of inflammatory myofibroblastic tumour of the bladder. Robotic enucleation enables excision of relatively large lesions with maximal bladder preservation.
Determinant features for surgical planning are tumour’s size and extent of exophytic growth. Small endophytic lesions can be managed successfully by transurethral resection. Exophytic lesions require more aggressive treatment in the form of partial or radical cystectomy depending on the size and the location of the lesion. In a systematic review by Teoh et al, of the 182 IMT patients, 60.8% were treated with TURBT, while 29.2% and 9.2% were treated with partial and radical cystectomy respectively [1].
Organ-sparing techniques should be considered whenever possible in IMT, given the relatively benign nature of lesion, and younger age group of affected population. Management of IMT requires a careful balance between adequate local excision to reduce the risk of any recurrence without sacrificing the bladder to maintain satisfactory functional capacity.
Robotic enucleation of bladder lesion has been previously described in management of bladder leiomyoma [7]. Enucleation allows the tumour to be completely excised en-bloc along its natural plane. In our case, enucleation was a feasible approach as adequate immunohistochemical staining pre-operatively confirmed IMT diagnosis and intraoperatively, the tumour was wellencapsulated with a distinct dissection plane and was located away from critical structures. At short term follow up, our patient remains recurrence-free on cystoscopy and crosssectional imaging and has no lower urinary tract symptoms, supporting the efficacy of enucleation in selected cases.
International Journal of Clinical & Medical Case Studies There is currently no established postoperative surveillance protocols for this condition. Risk factors for recurrence include larger tumour size, infiltrative histological features, and ALK gene rearrangements. Despite the overall low risk of progression, ongoing clinical surveillance remains important. Crosssectional imaging are recommended alongside cystoscopy surveillance to detect local recurrence, given exophytic growth pattern, which may be associated with a normal-appearing overlying urothelium. Imaging also facilitates assessment for regional or distant recurrence. While the optimal duration of follow-up is not well defined, we recommend surveillance for a minimum of five years.
Inflammatory myofibroblastic tumour of the bladder is a rare but potentially recurrent entity, often affecting young patients and posing a unique challenge in balancing oncological control with organ functional preservation. In select cases, a precise enucleation technique may offer a safe and effective alternative to radical surgery, particularly for well-circumscribed, moderate size exophytic lesions.